Downloaded 416 times























![ ROS can inhibit endothelium-dependent vasodilator
pathways [i.e. the NO pathway and the EDHF pathways]
and shift the balance in eicosanoids action from
vasodilation and antithrombosis toward vasoconstriction
and thrombosis.
Superoxide anions reduce the bioavailibility of NO,
inhibit its main target, soluble guanylyl cyclase, and
inactivate calcium-activated potassium channels.
Peroxynitrites inhibit guanylyl cyclase, superoxide
dismutases and decrease the EDHF component.](https://image.slidesharecdn.com/vascularendothelium-140415094925-phpapp01/75/Vascular-endothelium-26-2048.jpg)





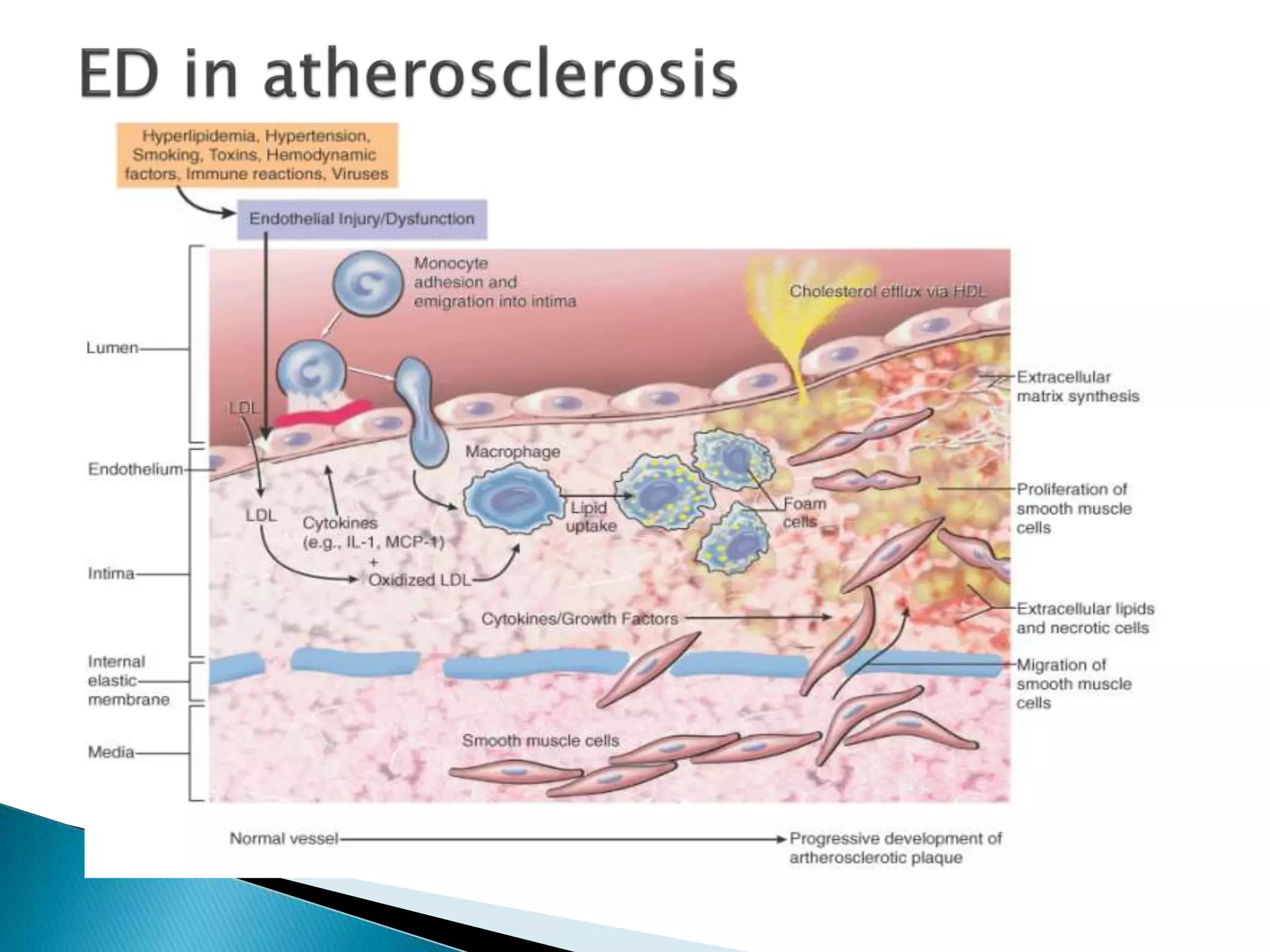





The document discusses the biology of vascular endothelium. It states that the endothelium is a thin layer of cells that lines the interior surface of blood vessels and lymphatic vessels, forming an interface between circulating blood/lymph and the vessel wall. The basic constituents of blood vessel walls are endothelial cells, smooth muscle cells, extracellular matrix, elastin, and collagen. The endothelium regulates vascular tone by releasing both vasodilators like nitric oxide, prostacyclin, and endothelium-derived hyperpolarizing factor and vasoconstrictors like endothelin-1 and thromboxane A2. Endothelial dysfunction, an imbalance between these factors, contributes to conditions like hypertension, atherosclerosis, and diabetes.











































































































