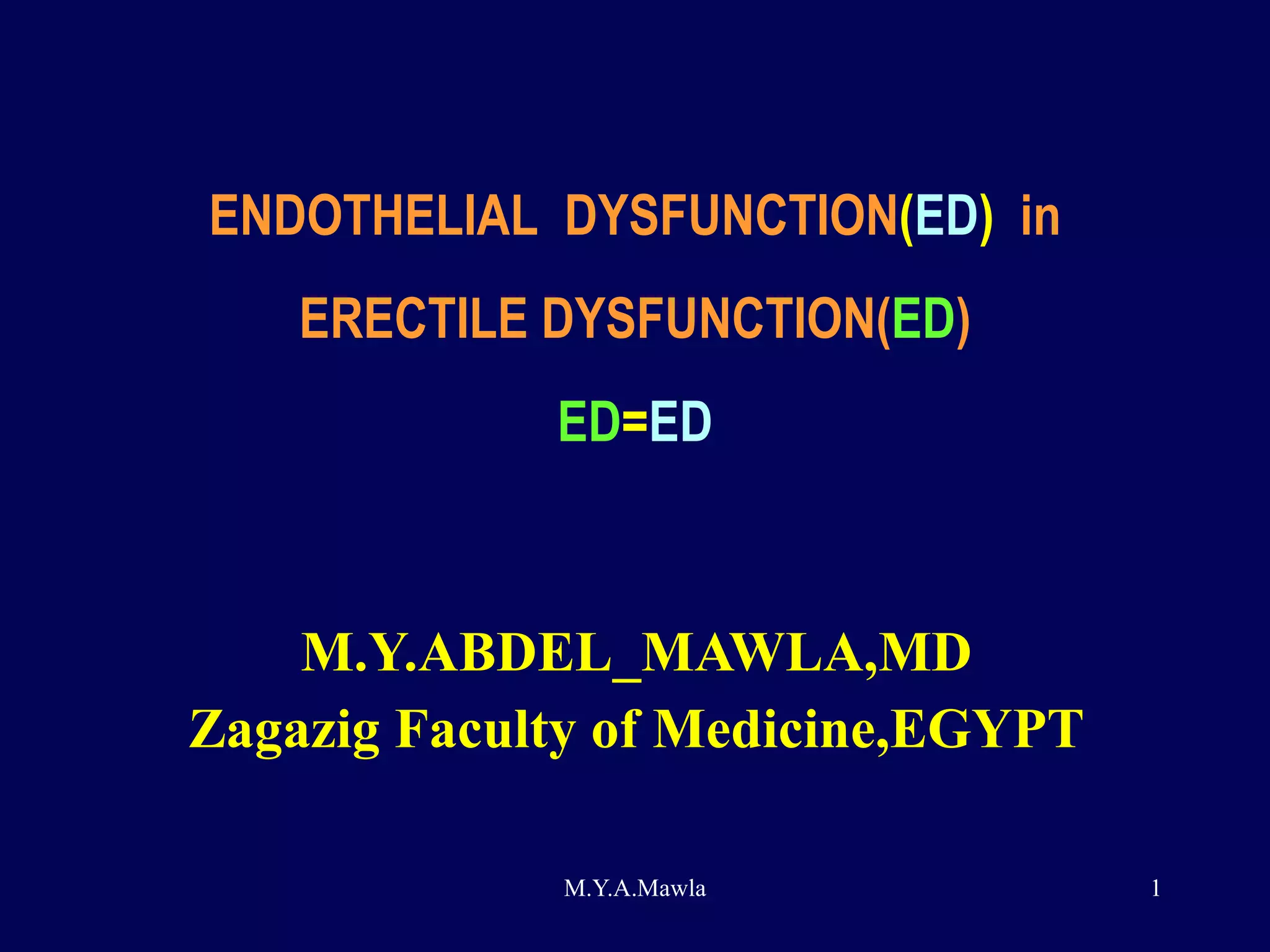
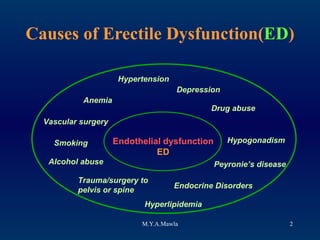
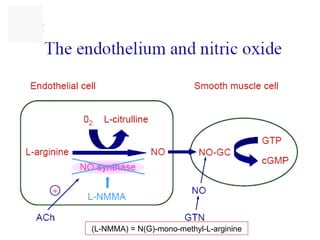
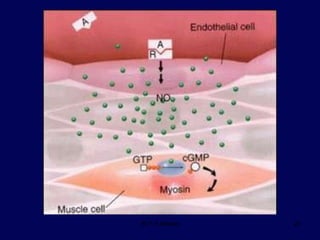
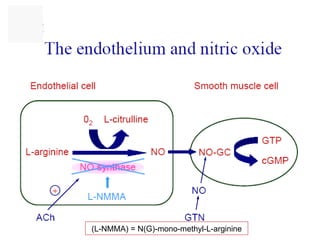
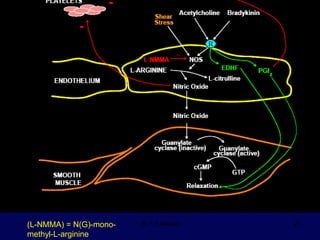
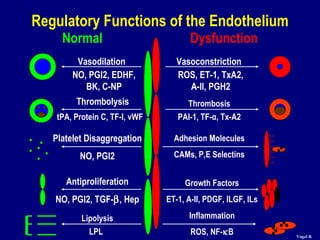
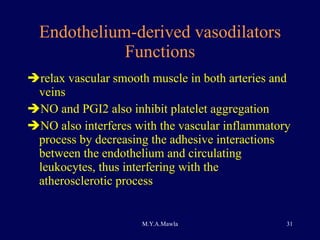
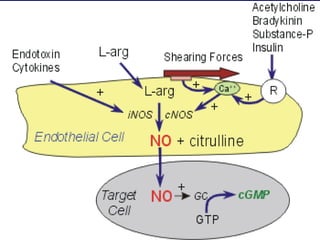
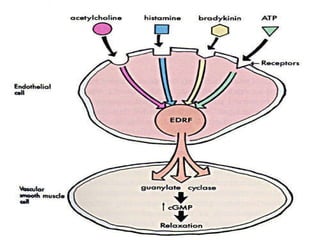
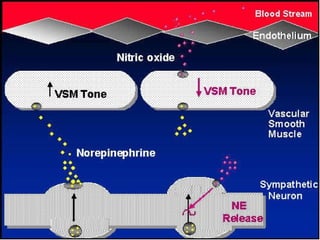
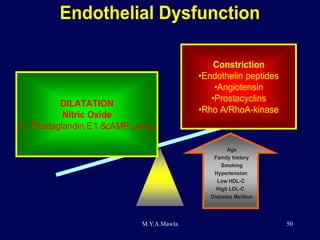
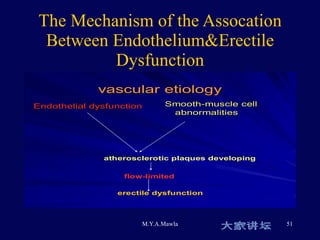
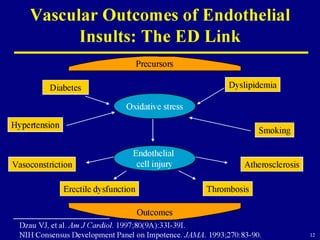
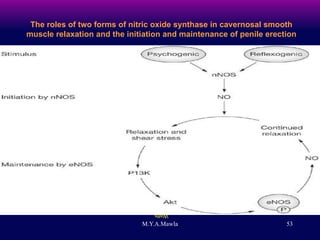
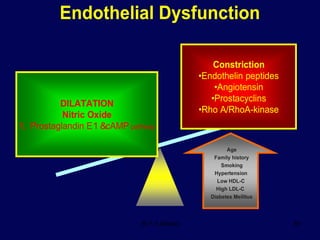
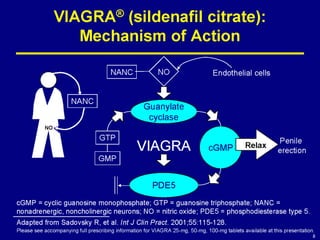
Endothelial dysfunction (ED) plays a central role in erectile dysfunction (ED). ED reduces the bioavailability of nitric oxide (NO), which is important for relaxation of the corpus cavernosum and penile erection. Risk factors for ED and endothelial dysfunction include diabetes, smoking, hypertension, hyperlipidemia, and other conditions that promote oxidative stress and reduce NO bioavailability.