Downloaded 320 times


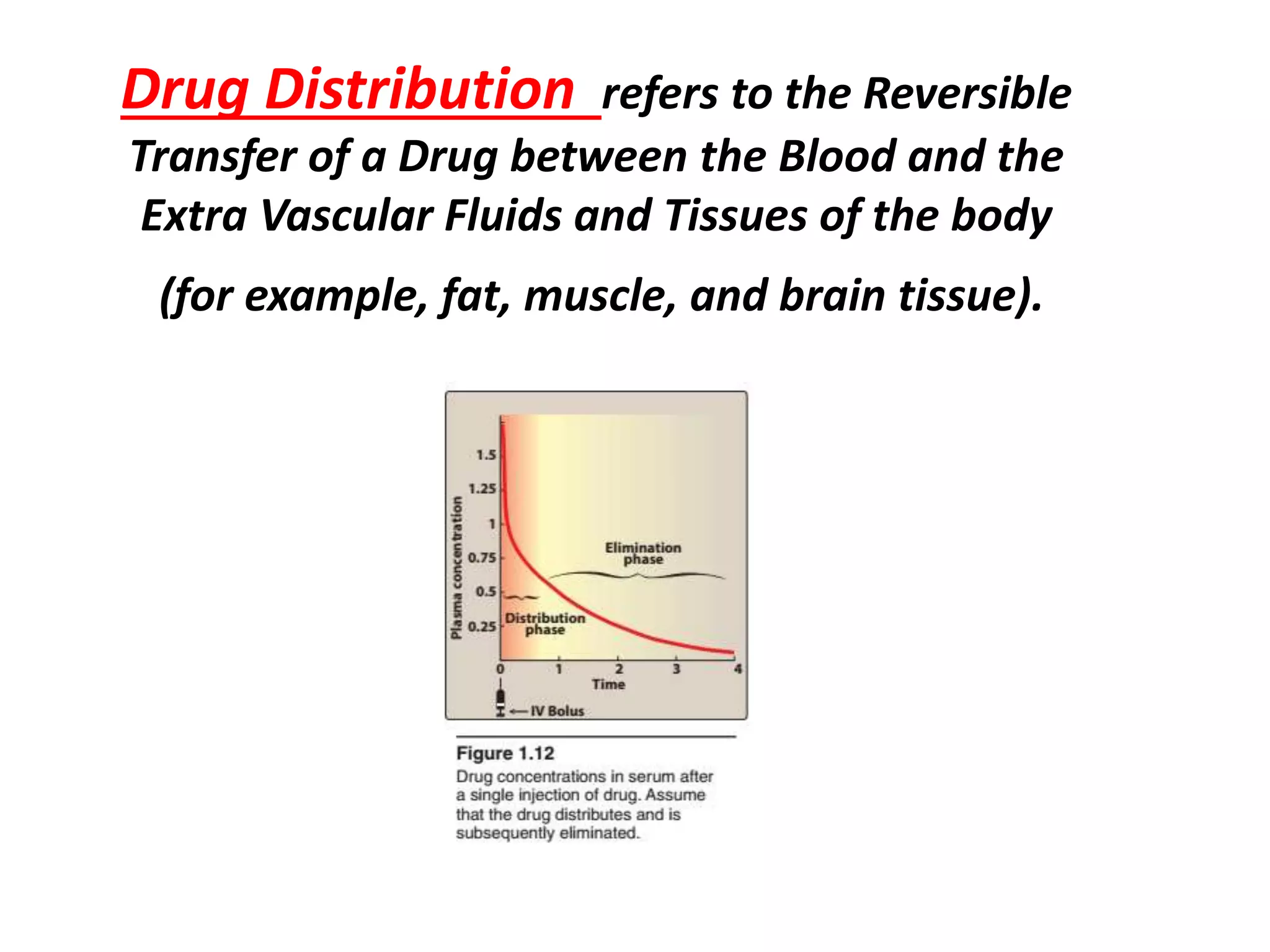





















1. The document discusses drug distribution between blood and tissues, factors affecting it like lipid solubility, and implications of volume of distribution, plasma protein binding, redistribution, and barriers like the blood-brain and placental barriers. 2. Apparent volume of distribution describes the fluid volume required to contain the entire drug dose at the same concentration as plasma, and is affected by factors like lipid solubility and plasma protein binding. 3. Plasma protein binding influences drug availability and can cause drug interactions through displacement, while barriers like the blood-brain and placental barriers control drug passage into sensitive tissues and the fetus.












![Clinical Pharmacokinetics-I [half life, order of kinetics, steady state]](https://cdn.slidesharecdn.com/ss_thumbnails/clinicalpk-ihalflifeorderofkineticssteadystate-140217020044-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)










































































