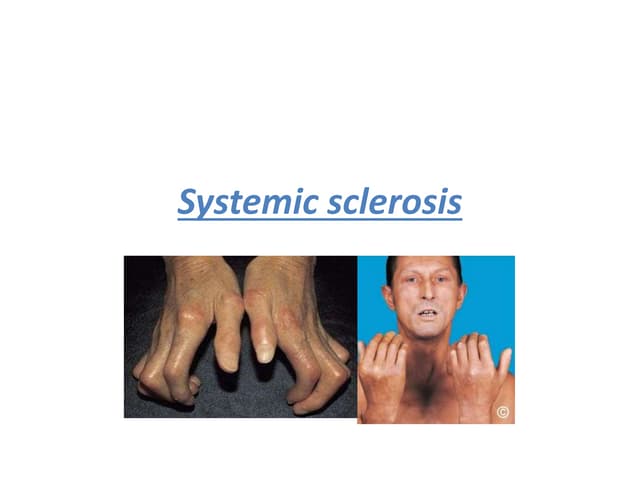
This case describes a patient with limited scleroderma (CREST syndrome). Key features include:
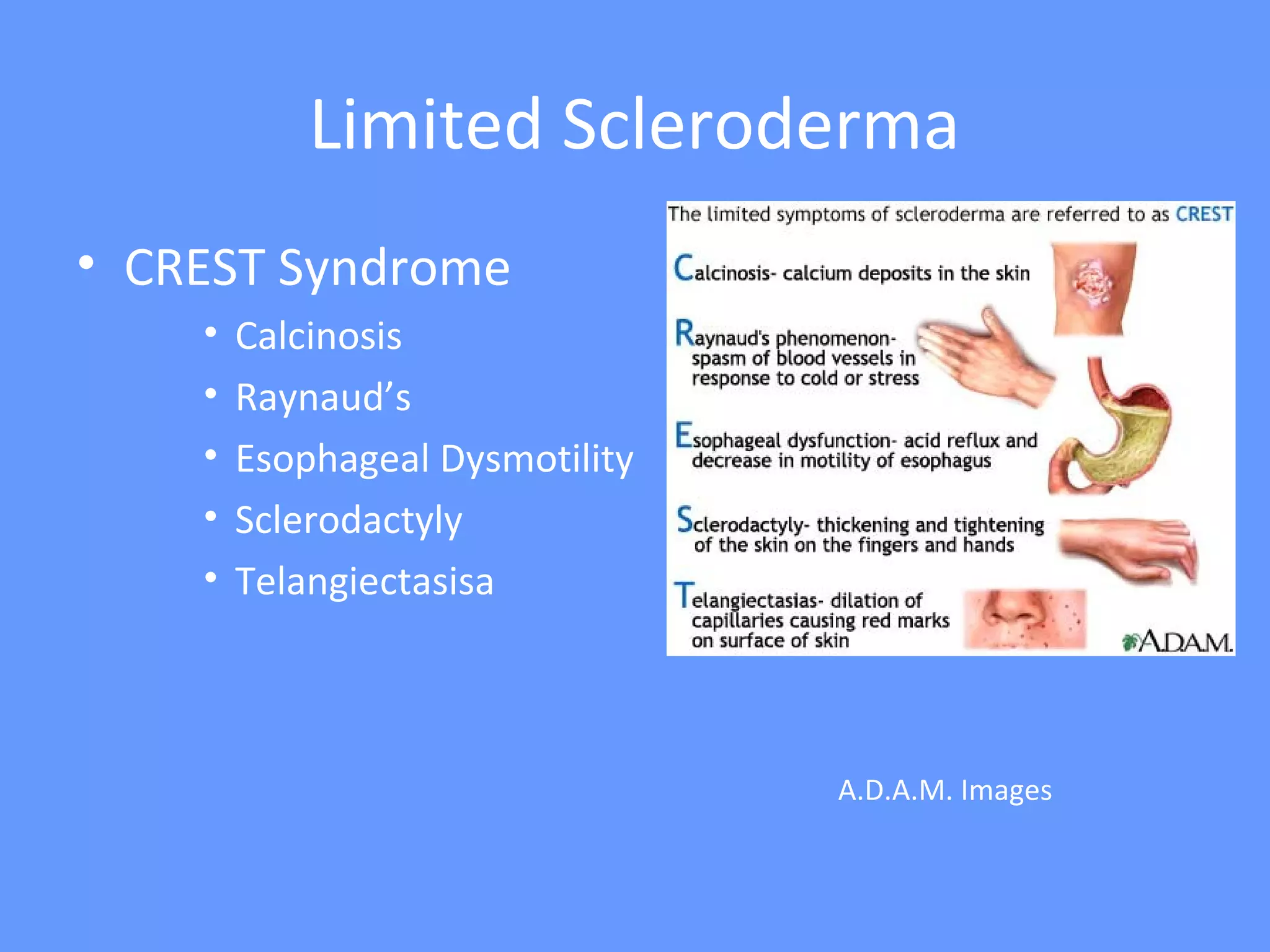
- A 50-year-old female with CREST syndrome characterized by calcinosis, Raynaud's phenomenon, esophageal dysmotility, sclerodactyly, and telangiectasias.
- She is positive for the autoantibody anti-centromere, which is seen in 70-80% of limited scleroderma/CREST syndrome cases.
- Her disease involves skin thickening distal to the elbows and knees (sclerodactyly), as well as gastrointestinal symptoms of esophageal dysmotility. She has minimal organ involvement typical of limited