Downloaded 2,316 times
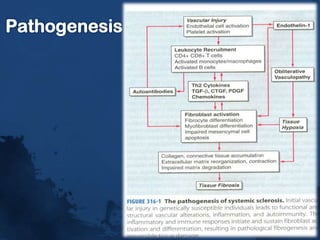
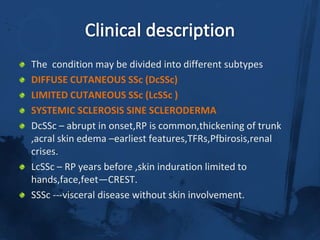
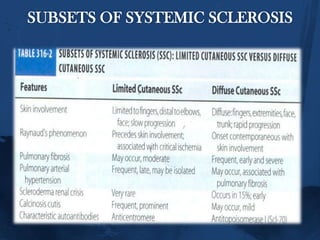
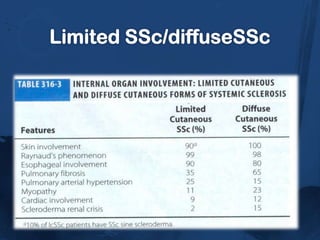
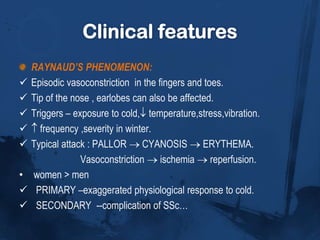
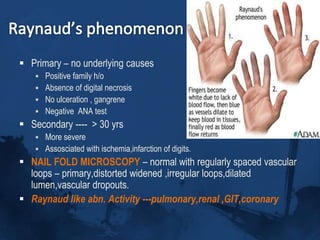
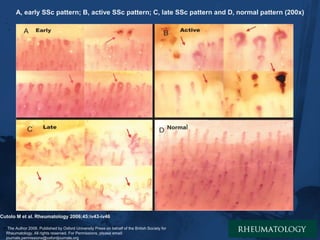




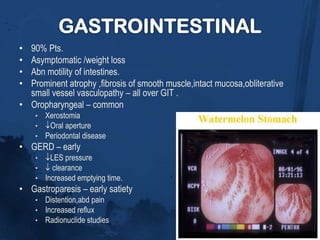
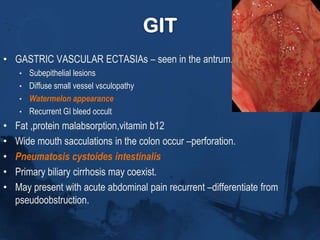


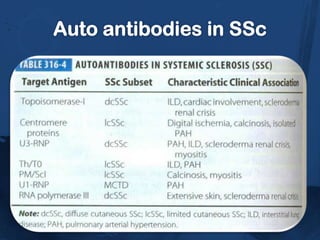
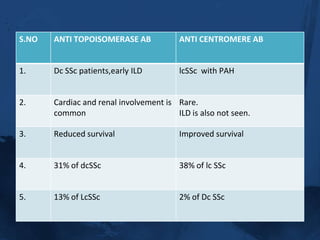

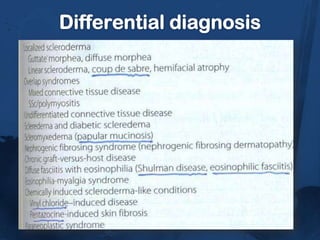
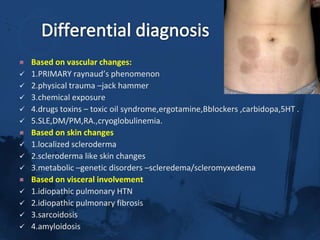




This document provides information on systemic sclerosis (SSc), a chronic autoimmune disease characterized by thickening and hardening of the skin, and involvement of internal organs. It can present as either limited or diffuse cutaneous forms. Key clinical features include Raynaud's phenomenon, skin thickening and tightening, digital pitting scars, and internal organ involvement such as interstitial lung disease, gastrointestinal issues, and renal crisis. Diagnosis involves clinical examination and the presence of autoantibodies. Differential diagnoses include other conditions presenting with similar skin or vascular changes. Complications can affect multiple organ systems and are a leading cause of mortality.



































































