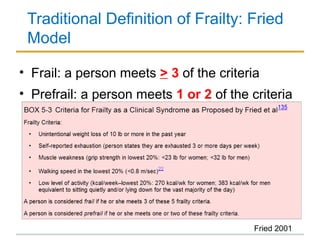
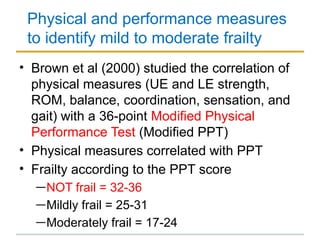
The document discusses the normal aging process and frailty syndrome. It defines old age as over 65 years and very old age as over 80 years. It describes the biological changes that occur with aging, including effects on important organ systems, and how aging makes it more difficult to handle physical stress. Frailty syndrome is defined as a condition resulting from the cumulative decline of multiple organ systems that increases vulnerability to stressors. Common features, consequences, and assessment methods are outlined.