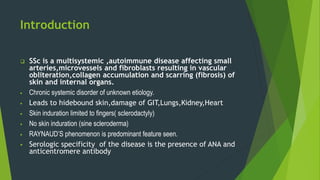
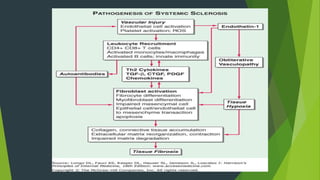
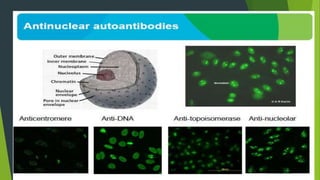
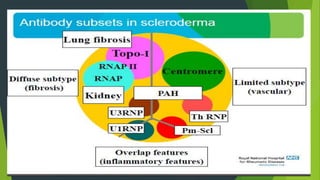
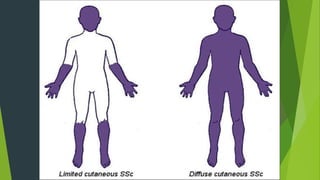
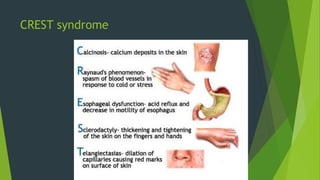
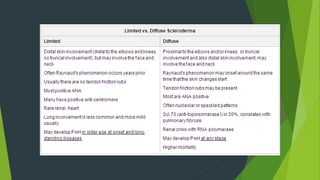
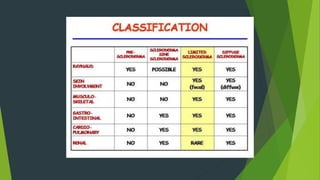
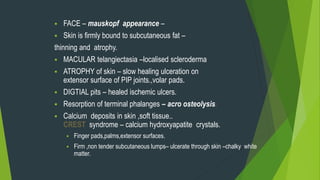
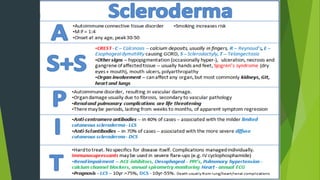
Systemic sclerosis, or scleroderma, is a rare autoimmune disease characterized by fibrosis of the skin and internal organs. It can be classified as either limited or diffuse cutaneous systemic sclerosis based on the extent of skin involvement. Common clinical features include Raynaud's phenomenon, skin thickening, gastrointestinal issues, lung fibrosis or pulmonary arterial hypertension, renal crisis, and calcinosis. The cause is unknown but likely involves environmental triggers in genetically susceptible individuals leading to endothelial cell dysfunction, inflammation, and excessive collagen deposition in affected tissues.















































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)














