Downloaded 92 times
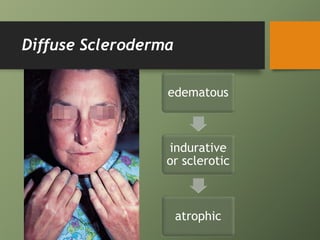

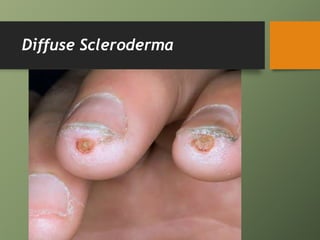
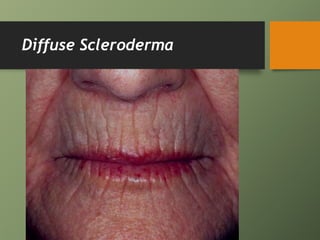
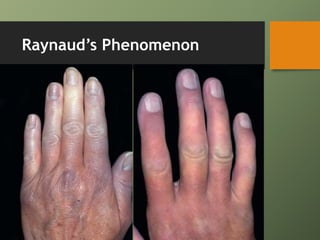
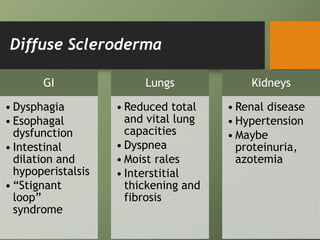
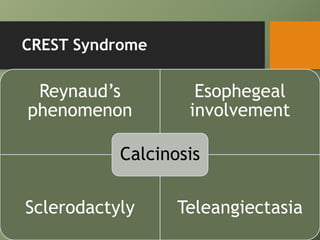


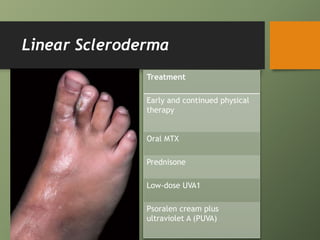
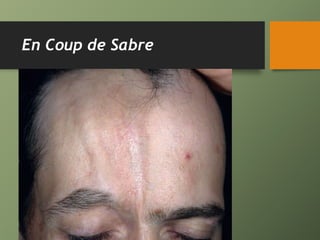

Scleroderma is a disease characterized by hardening and tightening of the skin and internal organs. It exists in both systemic and localized forms. Systemic scleroderma can be diffuse, affecting much of the skin and internal organs early on, or CREST syndrome, which more commonly causes limited skin hardening and internal organ issues later. Localized scleroderma includes conditions like morphea that cause hardened plaques of skin. Treatment depends on the specific type but may include medications, physical therapy, phototherapy, and moisturizers.








































































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)














