Downloaded 310 times









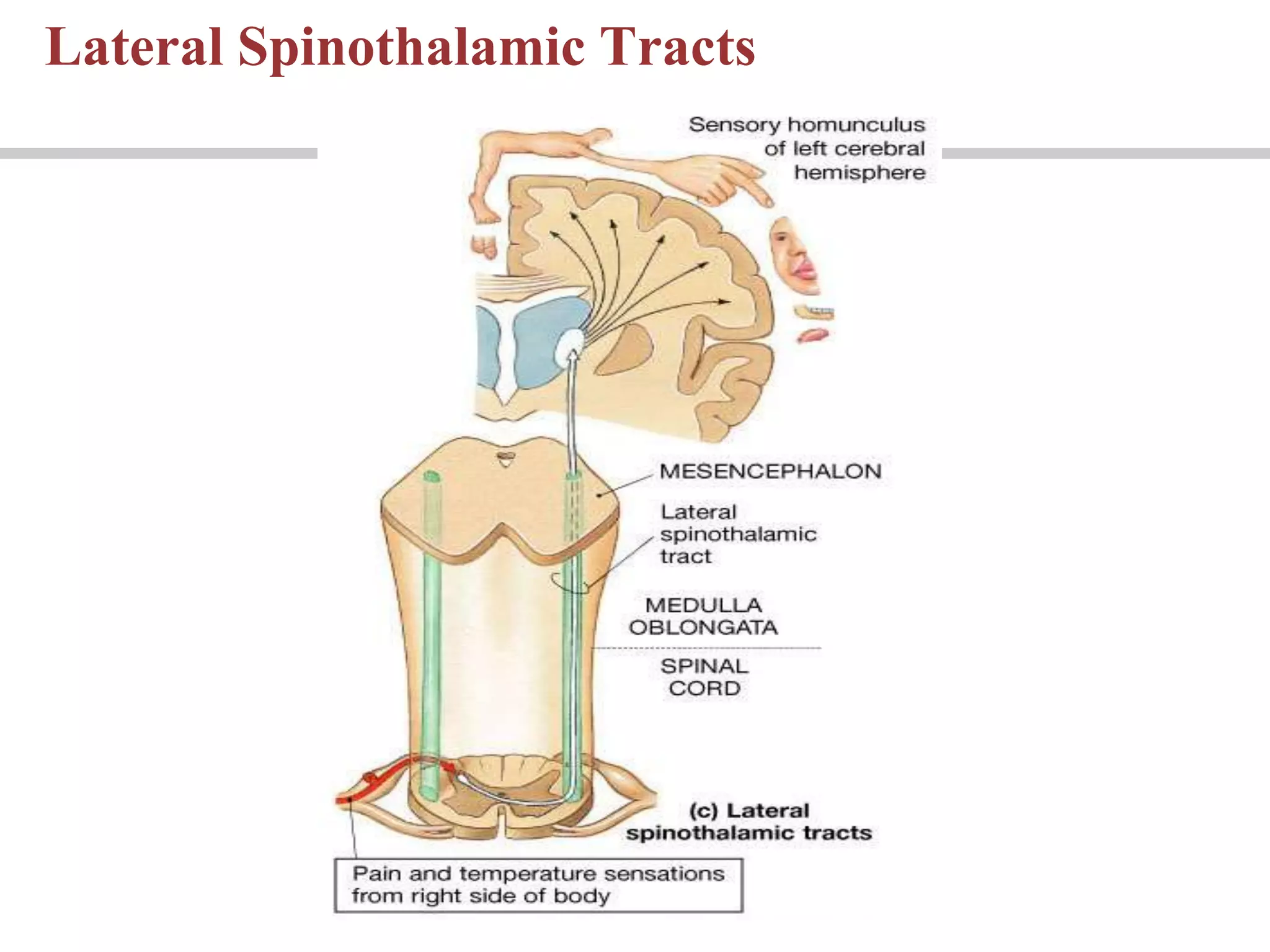

































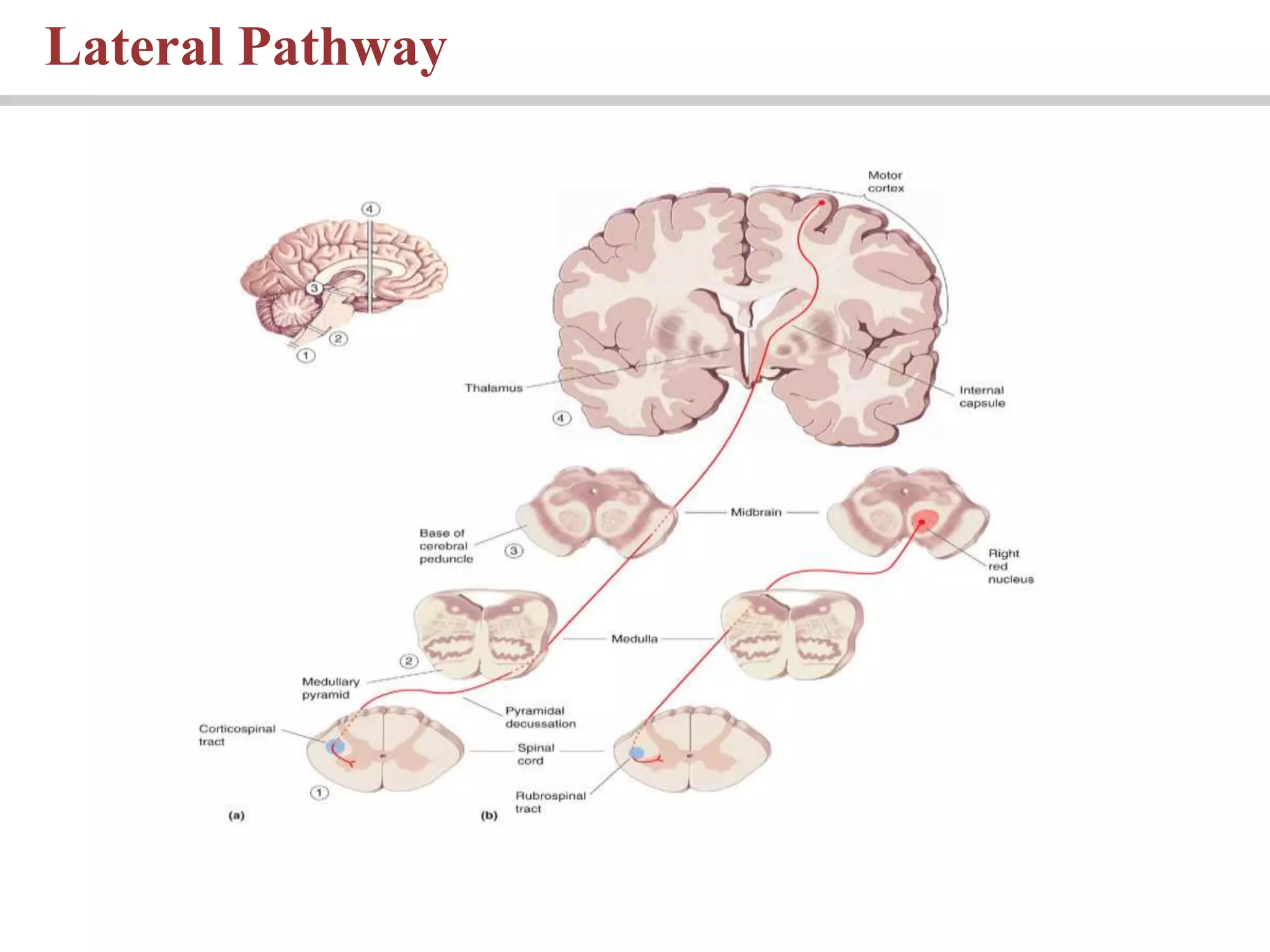









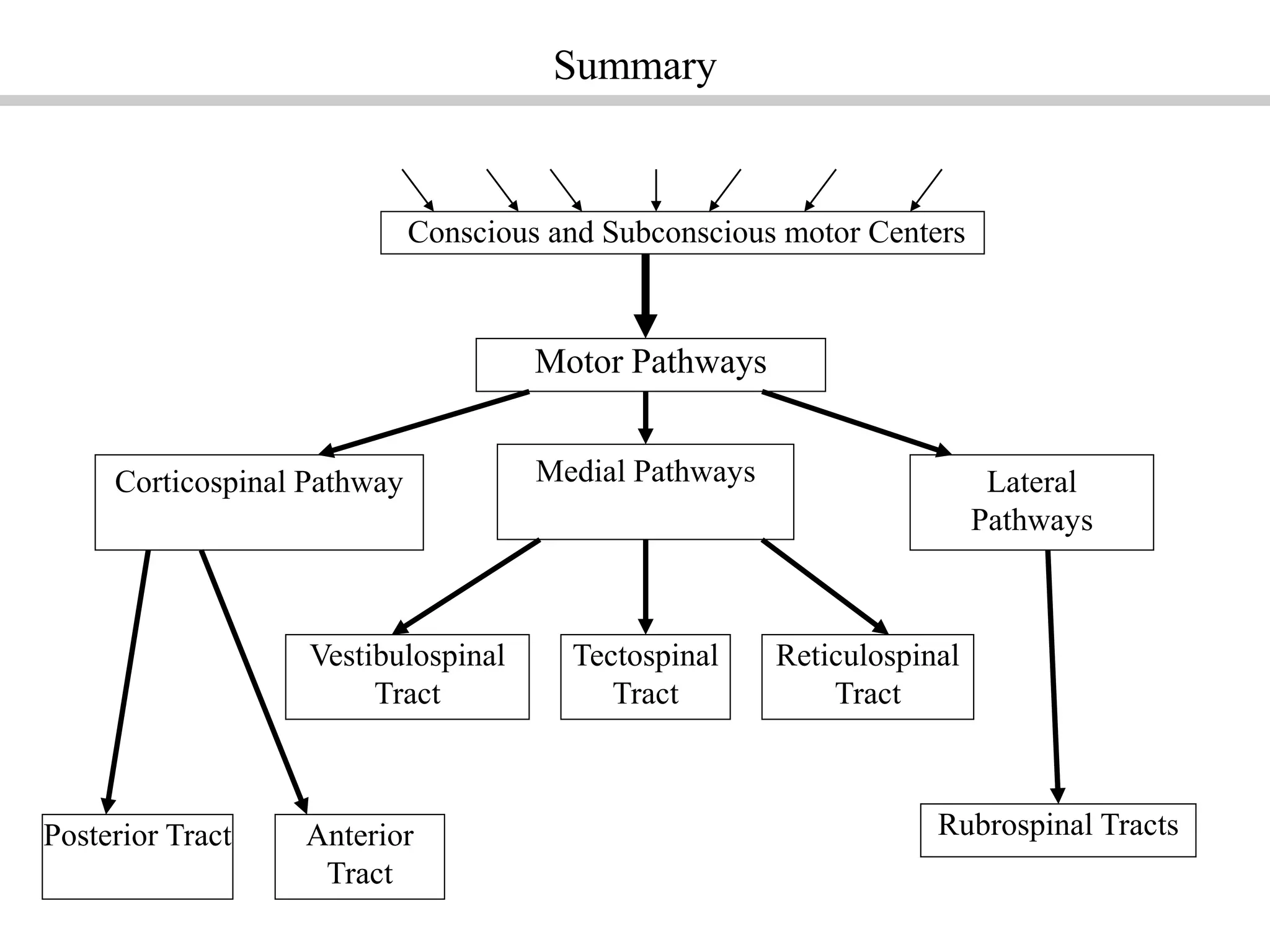





























1) The motor cortex and corticospinal tract provide conscious control of voluntary skeletal muscle movements. The corticospinal tract contains fibers that cross to the opposite side of the body and fibers that remain on the same side. 2) Sensory information travels through ascending tracts in the spinal cord including the posterior, lateral, and spinocerebellar tracts to the brain. 3) The medial and lateral motor pathways issue subconscious motor commands through tracts like the rubrospinal and reticulospinal tracts to control gross movements and posture.
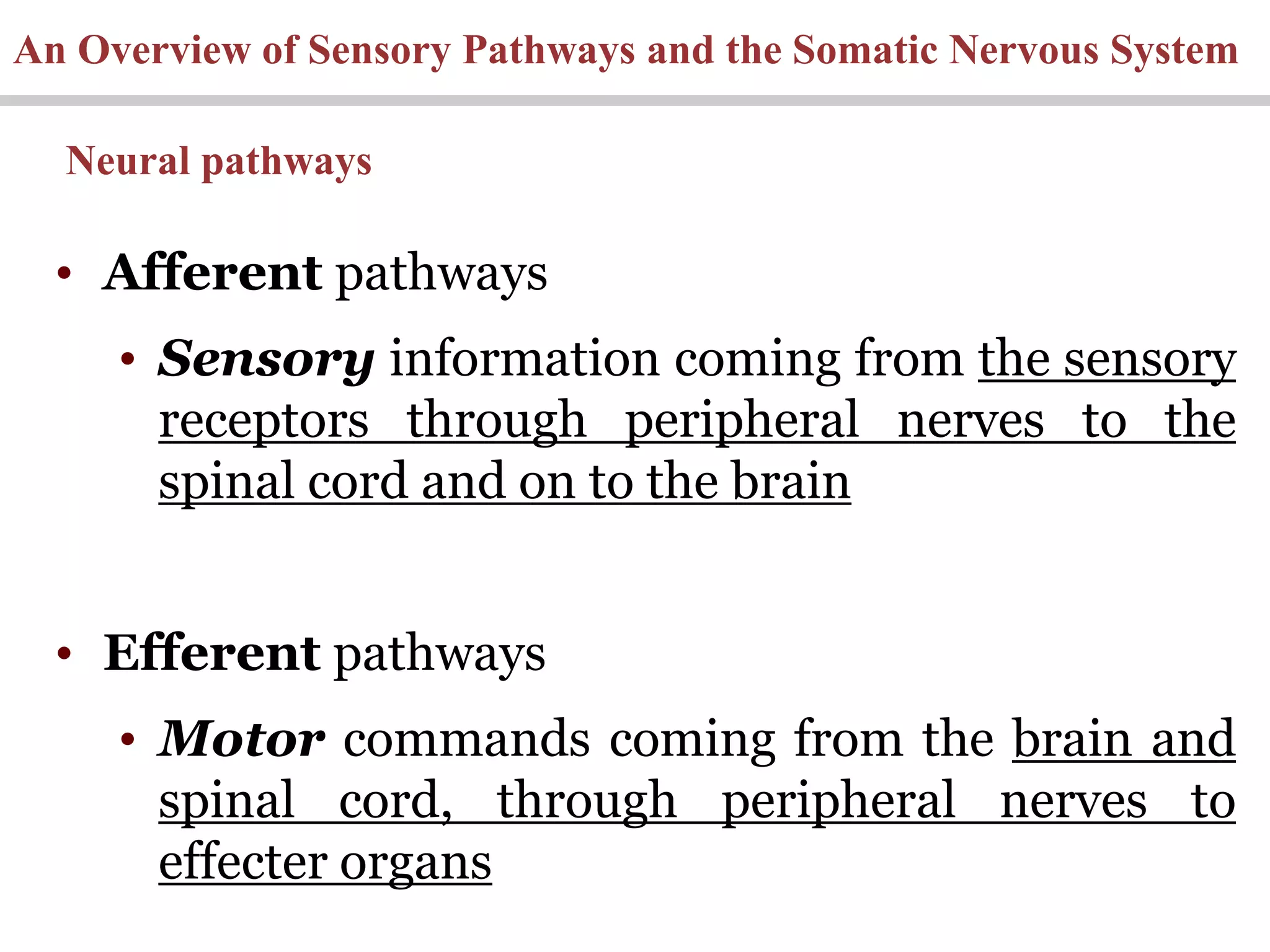
Introduces the motor system, sensory pathways, and somatic nervous system with neural integration.
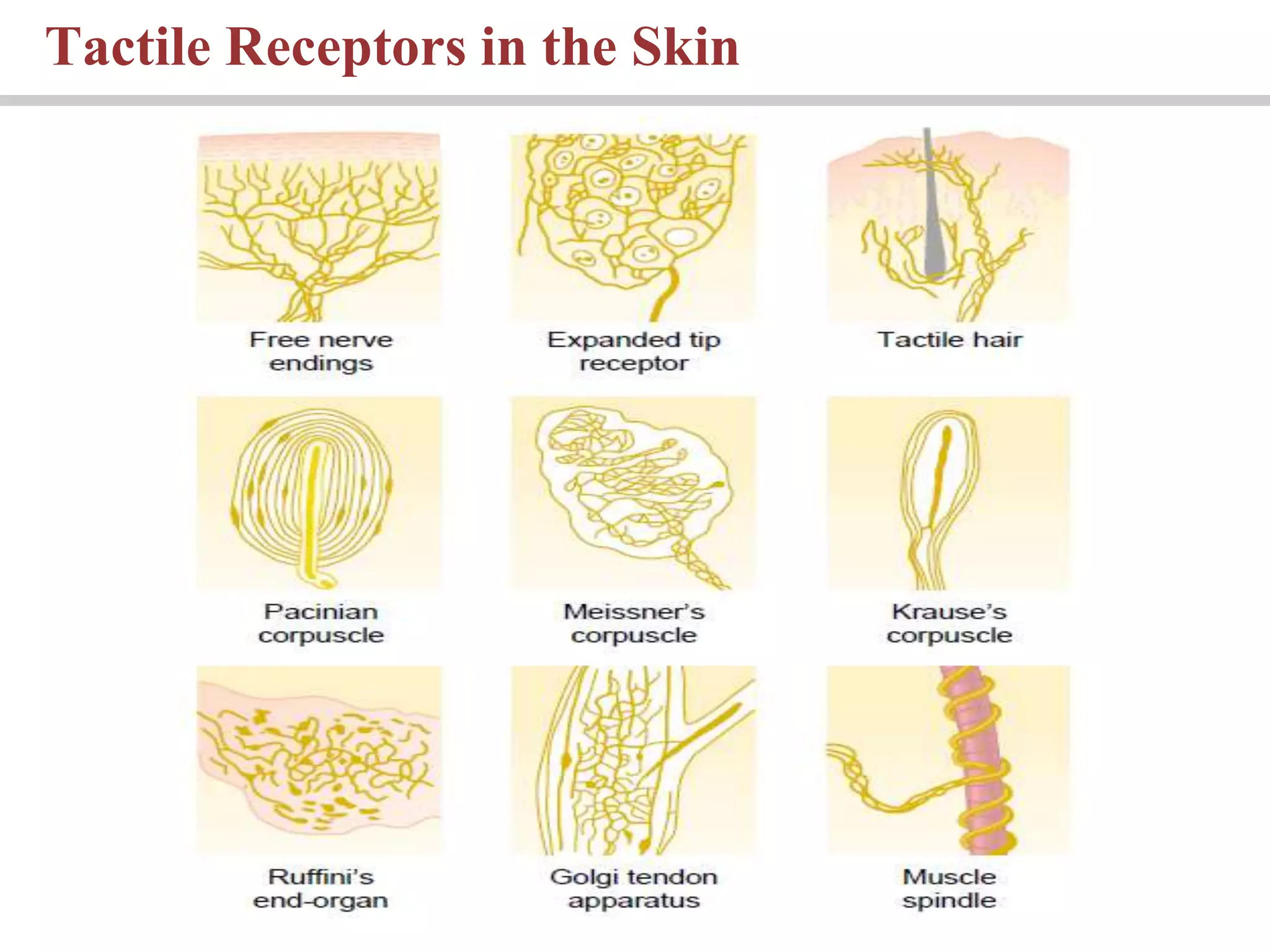
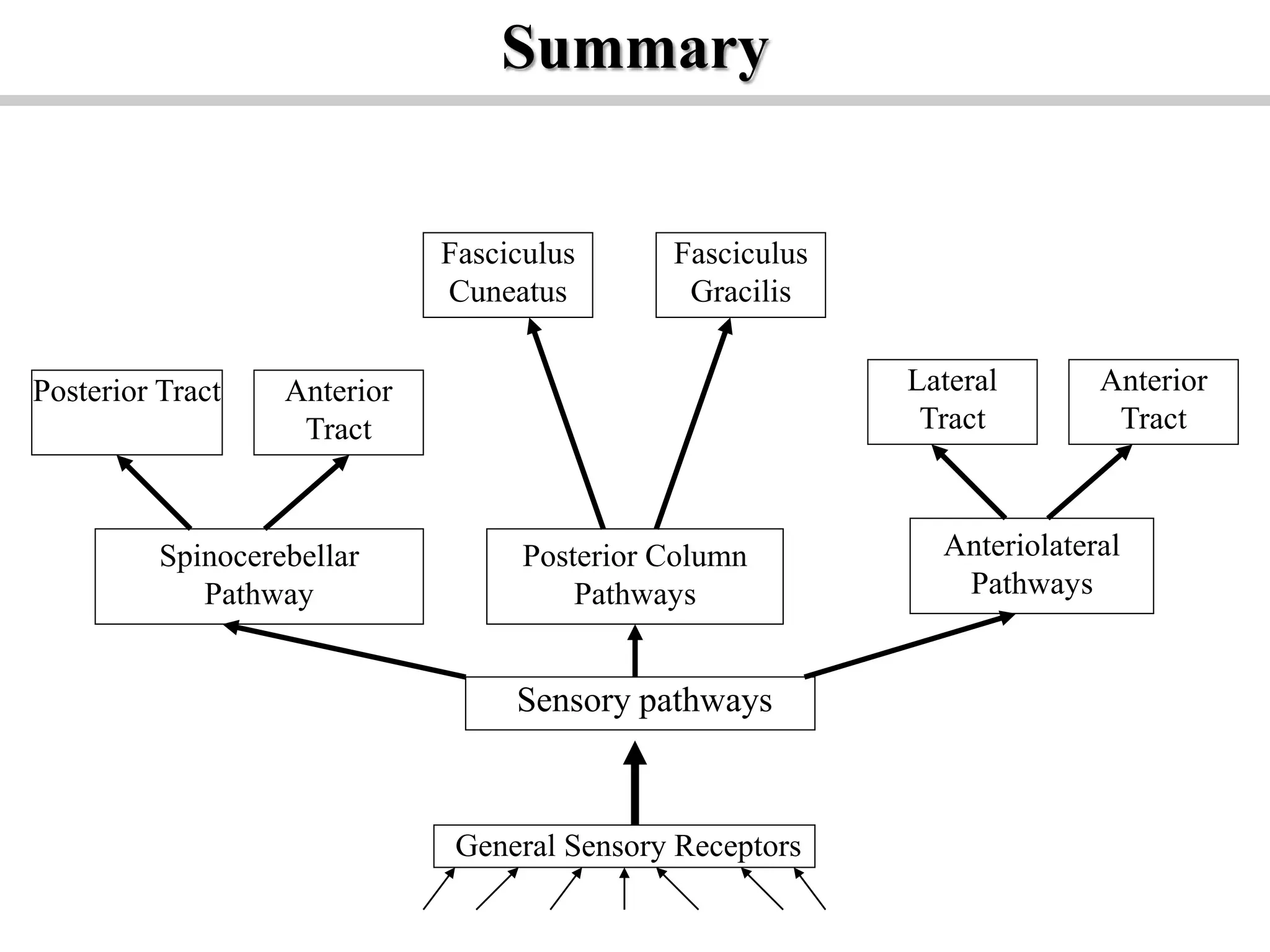
Details sensory receptors, types of neurons, and sensory pathways including posterior column, anterolateral, and spinocerebellar pathways.
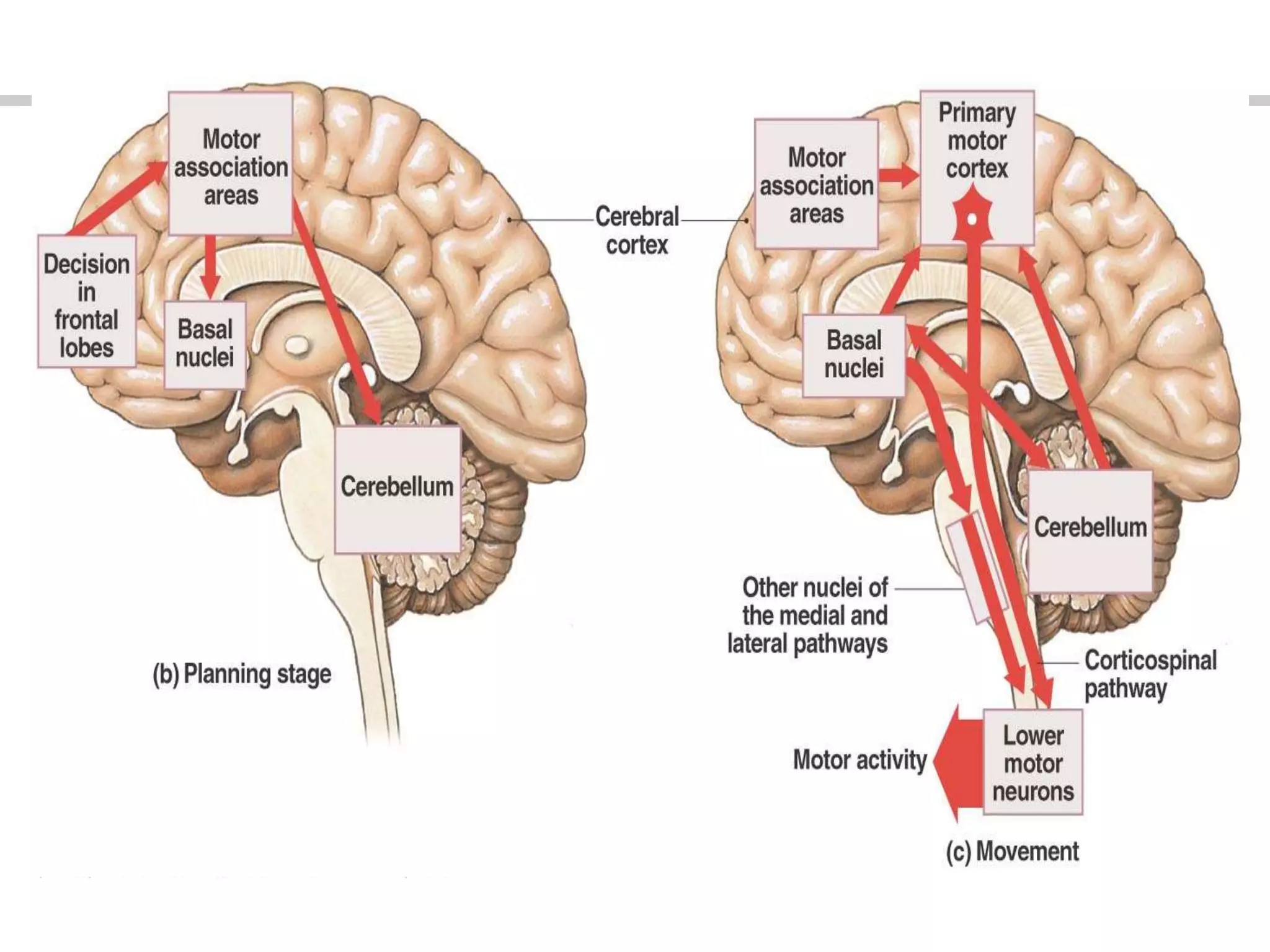
Levels of motor control: highest (motor cortex), middle (subcortical centers), lowest (spinal cord) and details about the motor cortex areas.
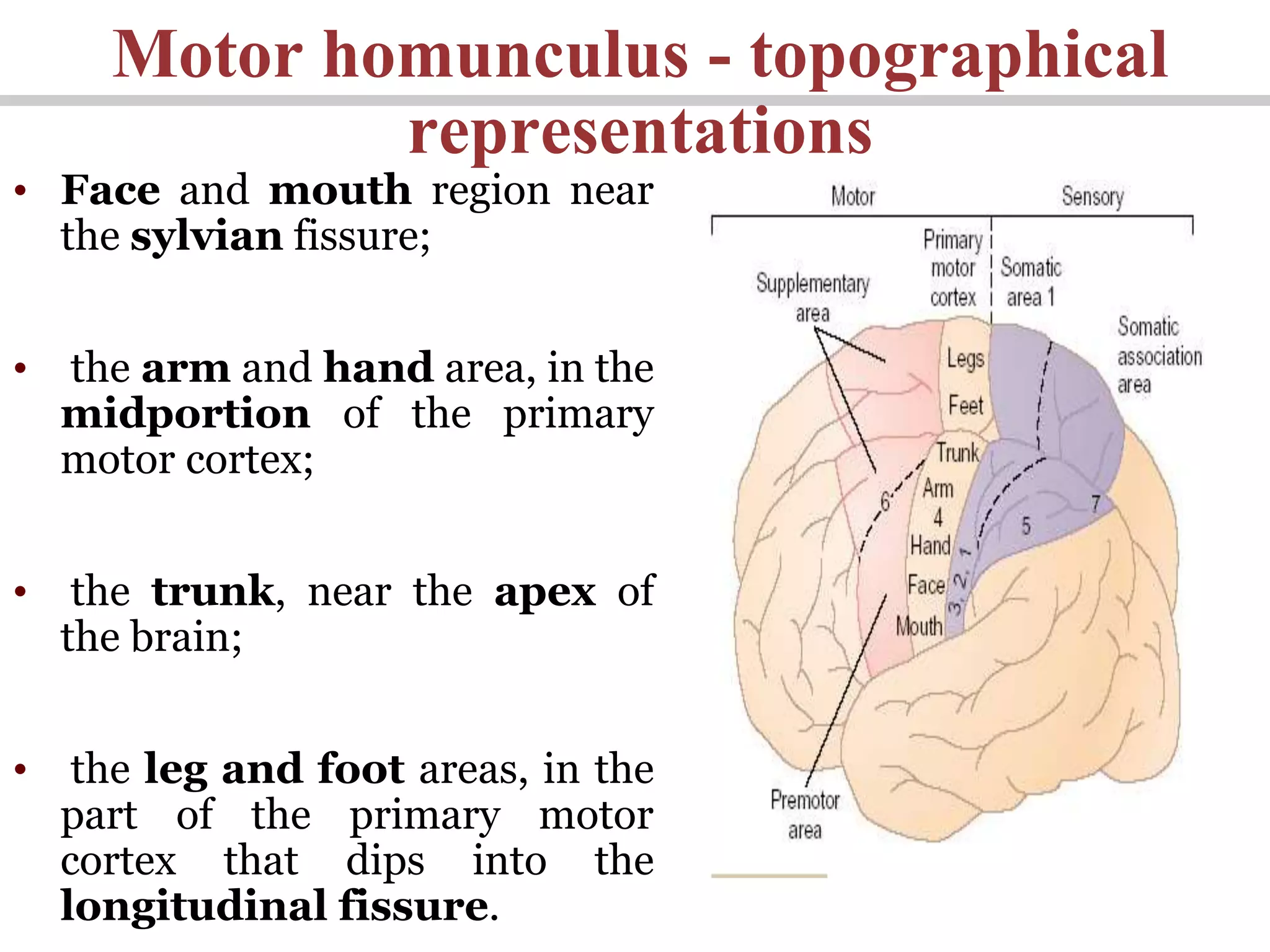
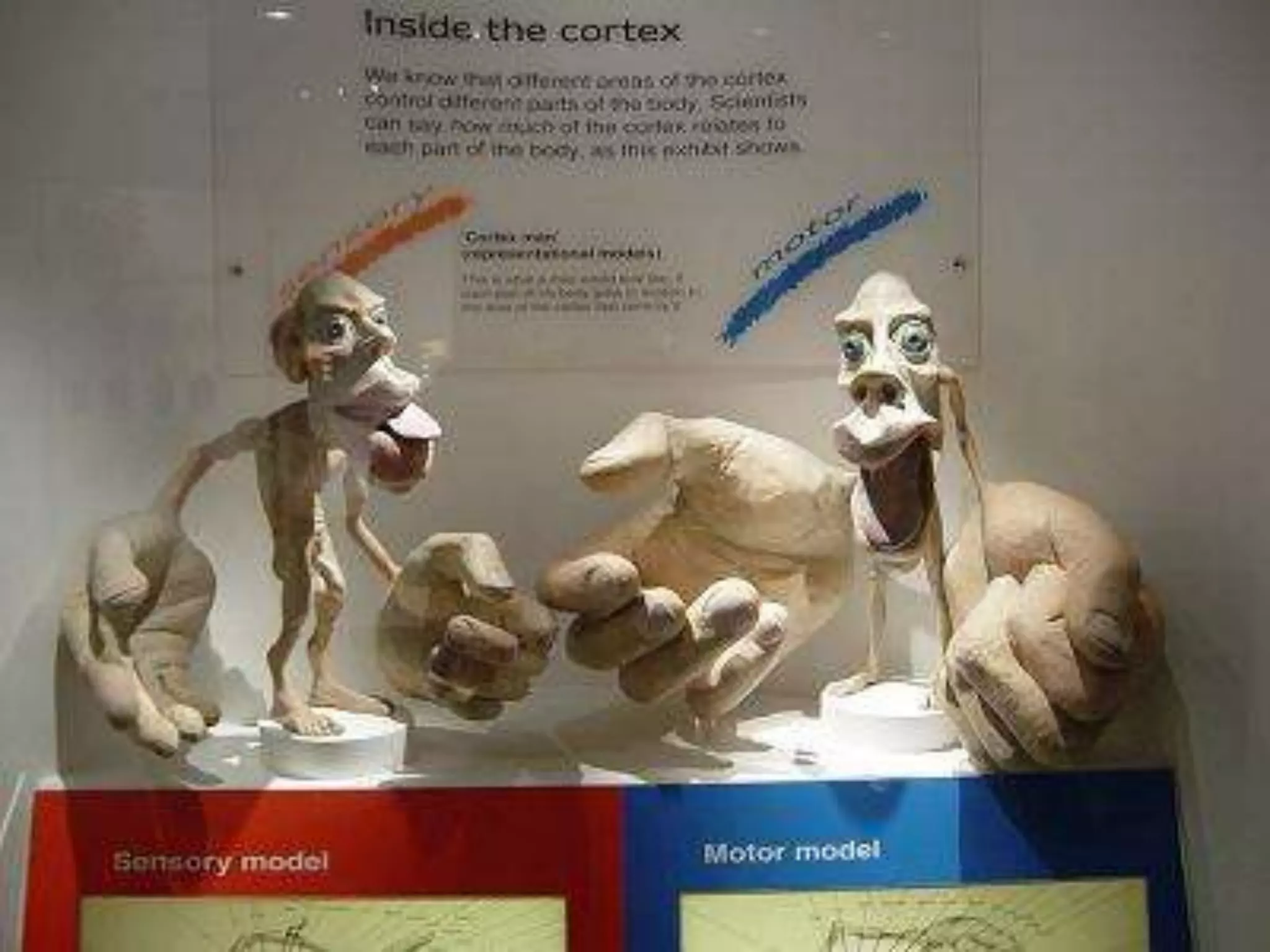
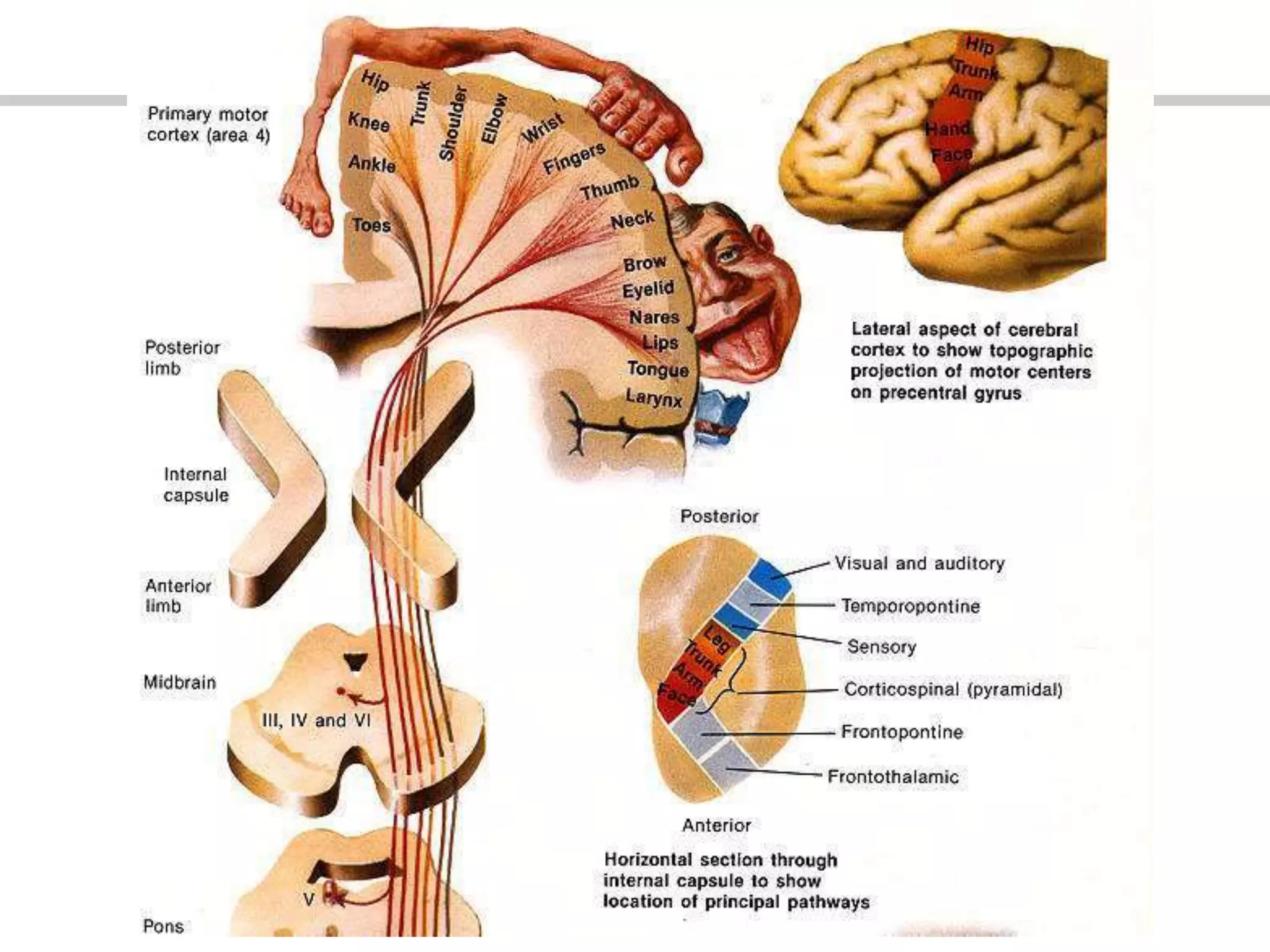
Explains motor homunculus, specialized areas for functions like speech, eye movement, and hand skills.
Describes descending motor tracts: pyramidal and extrapyramidal tracts, their structure and importance in voluntary movements.
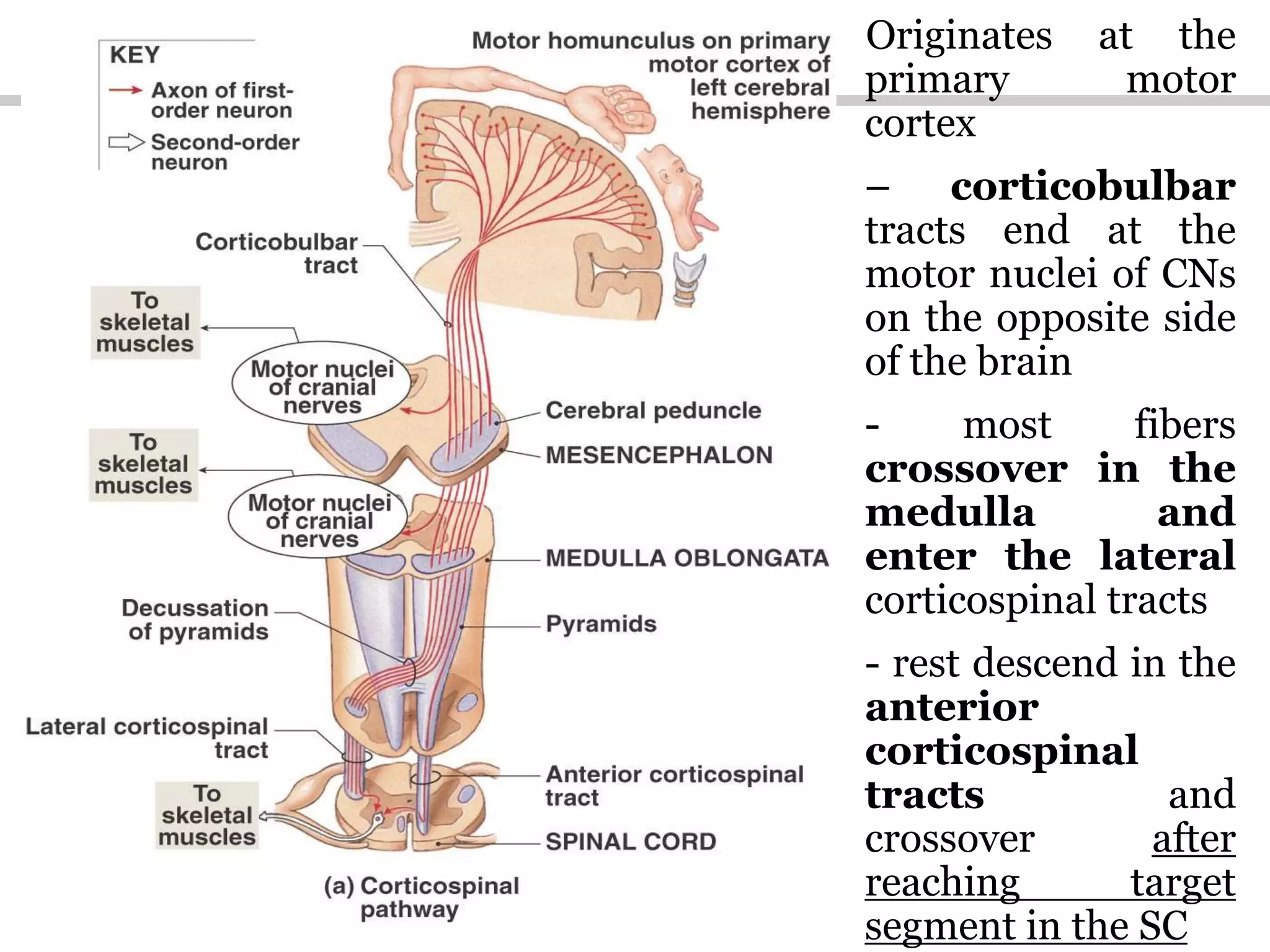
Explains the internal capsule, the function of corticospinal tracts, their terminations, and lesion impacts.
Discusses symptoms and impacts of upper motor neuron and lower motor neuron lesions involving paralysis and reflexes.
Introduces somatic and autonomic systems, detailing descending tracts and their control over muscular movements.
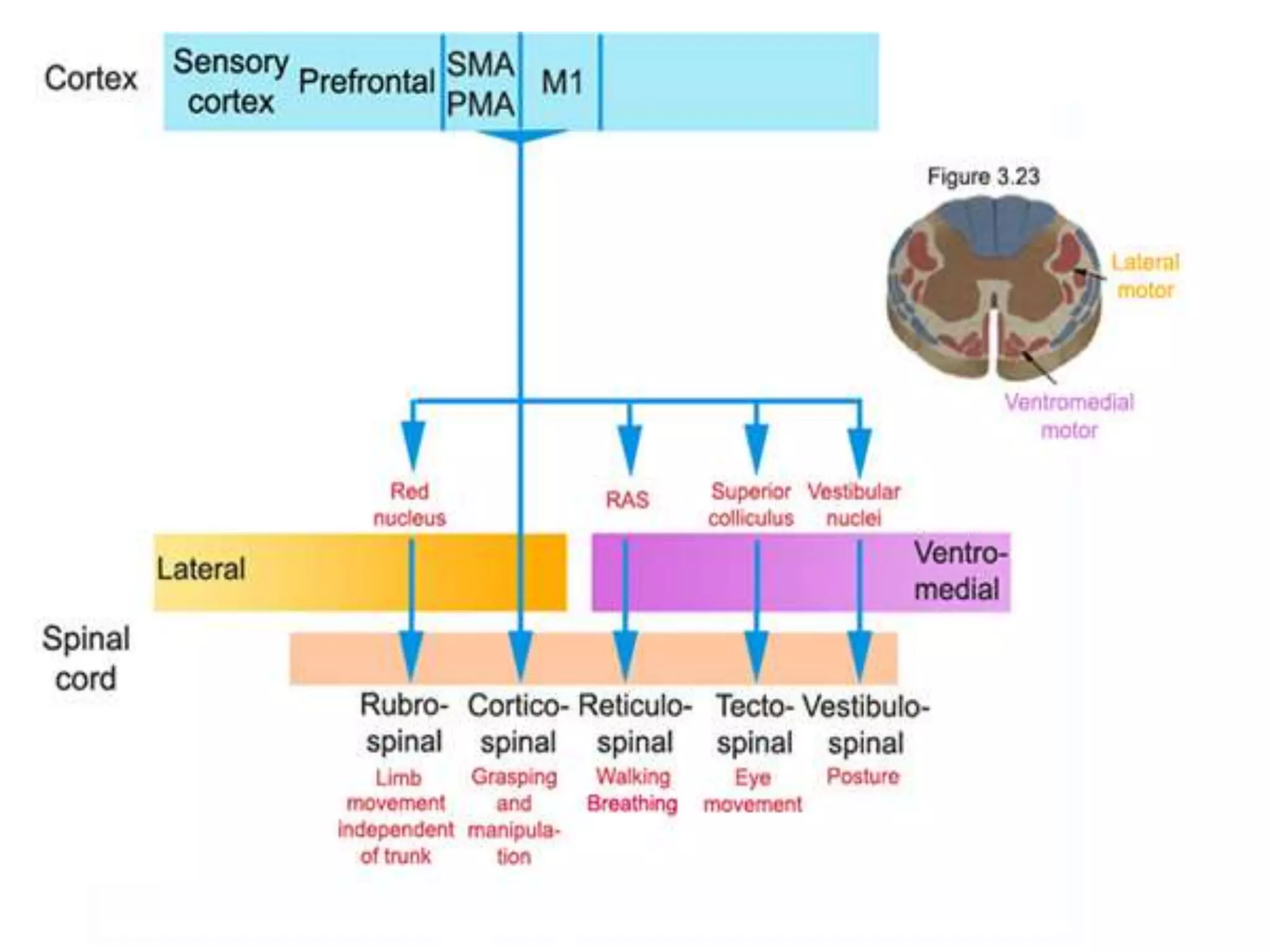
Explains the roles of the extrapyramidal system including reticulospinal, vestibulospinal, and tectospinal tracts in coordination and posture.
Discusses decerebrate rigidity, its features, and physiological impacts on muscle control strength.
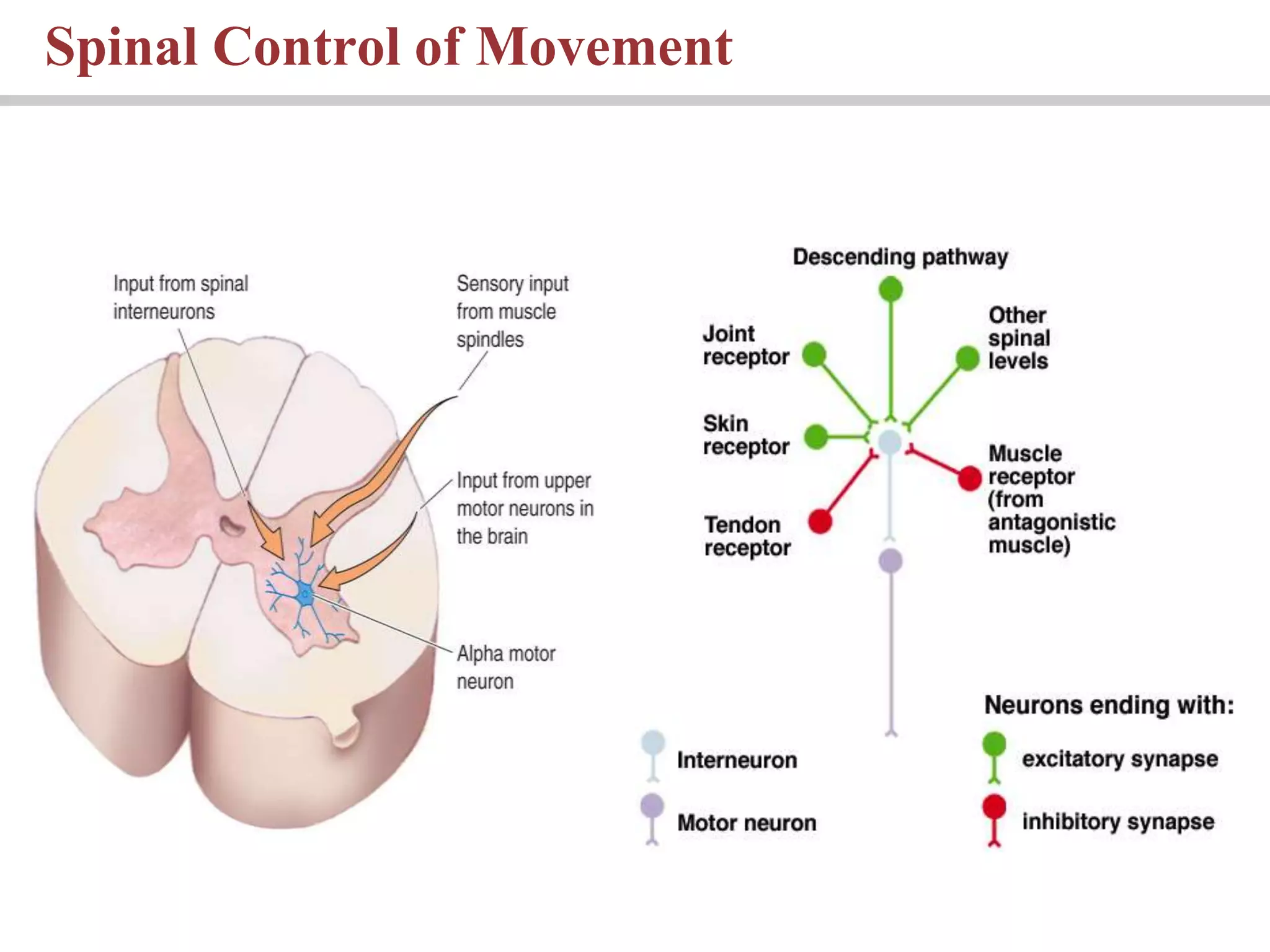
Summarizes spinal and brain control of movement, illustrating functional areas of the cerebral cortex.























































































