Downloaded 77 times
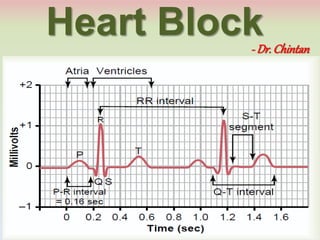


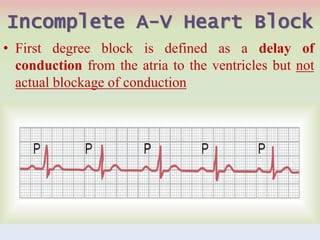






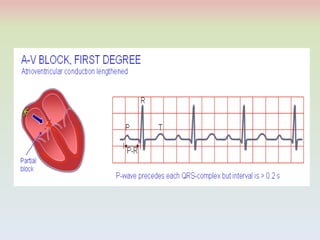


























This document discusses different types of heart block. It describes sinoatrial block where the impulse from the sinus node is blocked before entering the atria. It also describes atrioventricular block where the impulse is blocked from passing from the atria to the ventricles. There are three degrees of atrioventricular block: first-degree with a prolonged PR interval, second-degree with intermittent conduction, and third-degree with persistent nonconduction. Causes of atrioventricular block include ischemia, compression, inflammation, and vagus nerve stimulation. Symptoms of complete heart block include dissociation of P waves and QRS complexes on ECG.























































































