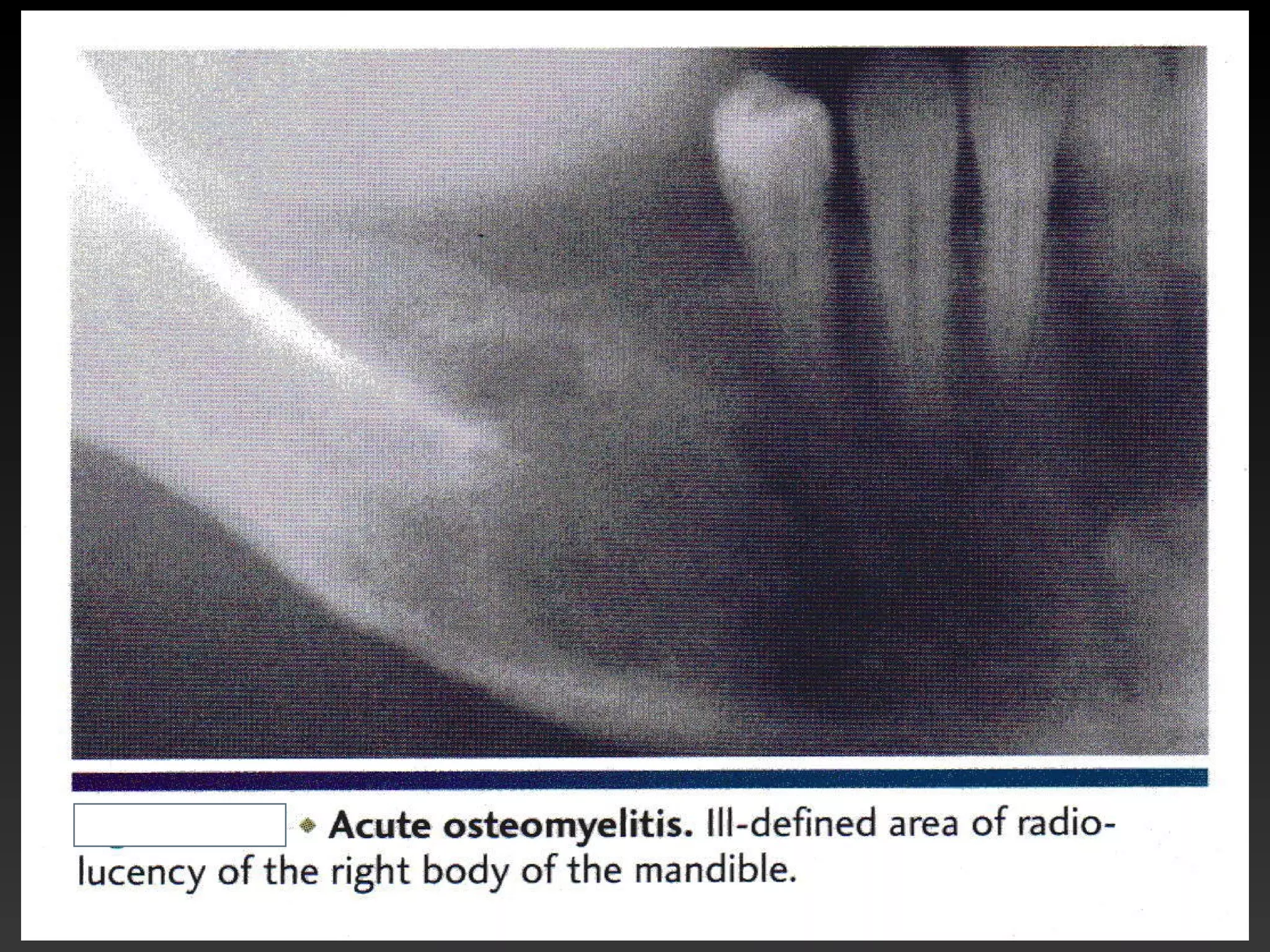
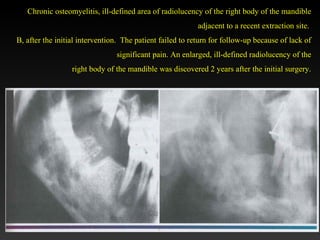
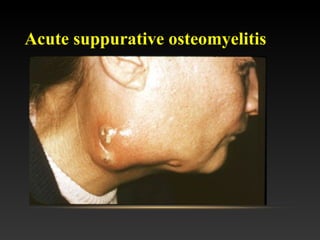
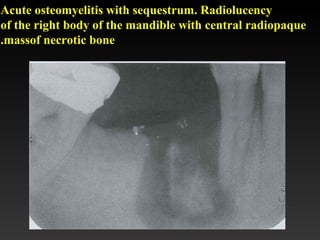
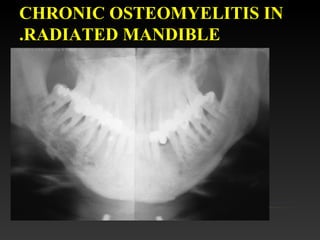
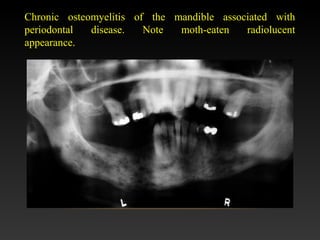
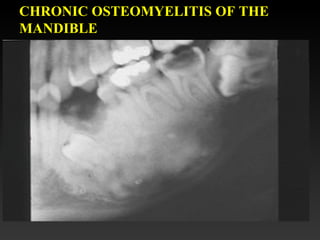
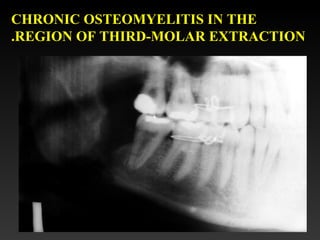
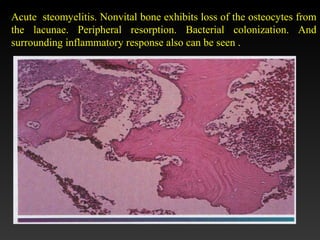
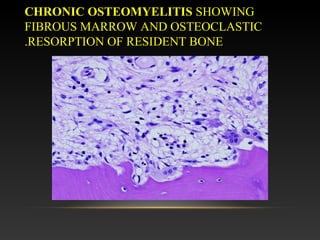
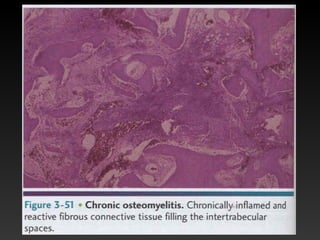
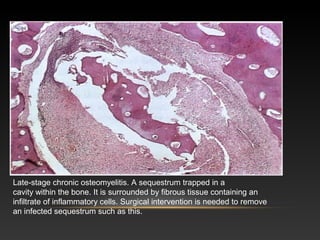
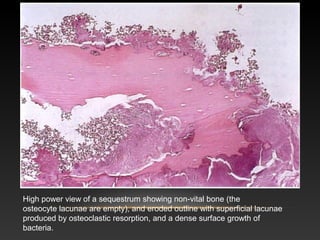
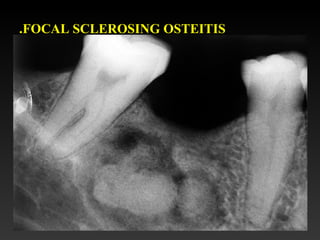
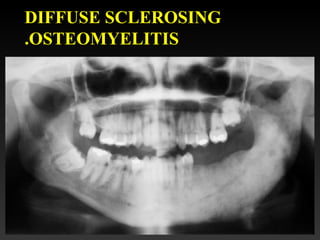
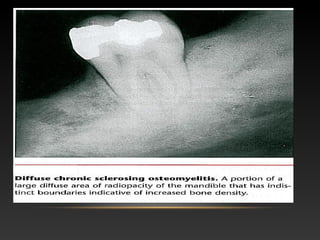
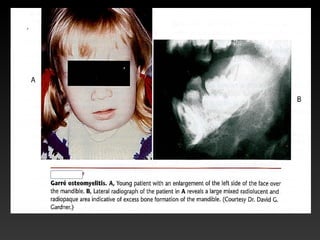
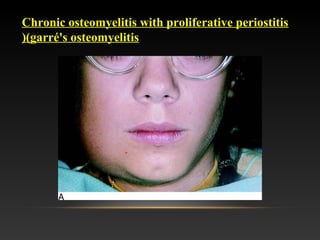
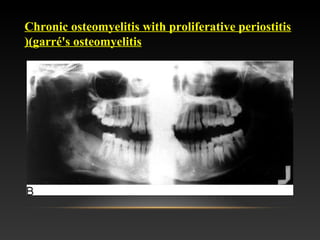
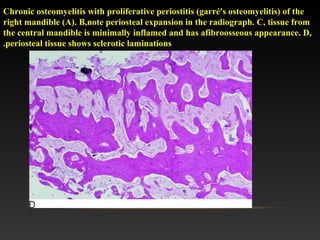
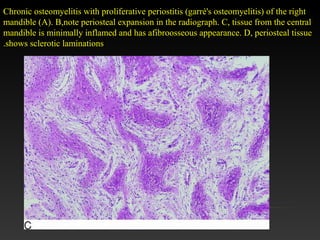
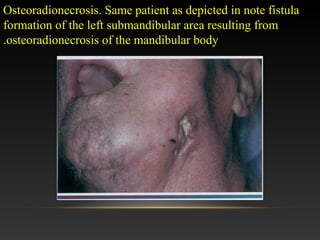
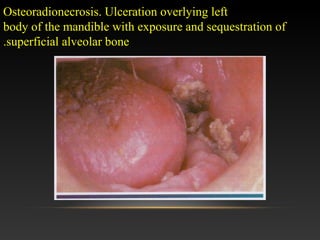
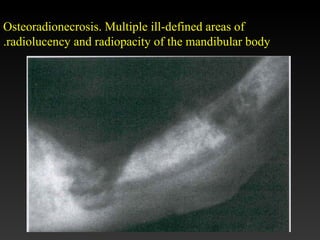
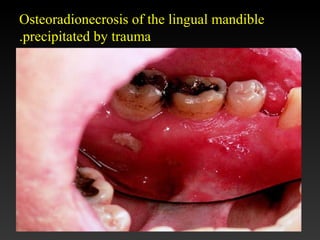
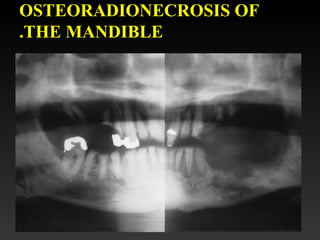
This document contains descriptions and images of various bone infections and conditions in the mandible, including osteomyelitis, osteoradionecrosis, and dry socket. Osteomyelitis is described as both acute and chronic, with features like non-vital bone, peripheral resorption, and bacterial colonization. Images show ill-defined radiolucencies and sequestra of necrotic bone. Osteoradionecrosis is characterized by ulceration and exposure of bone following radiation therapy. Dry socket is identified by an empty tooth socket with the bony lamina dura visible.









































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)
![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)















