Downloaded 13 times


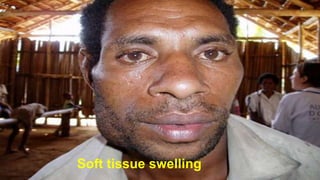


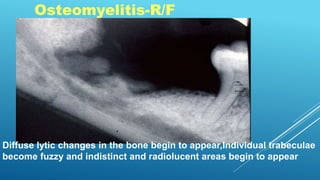
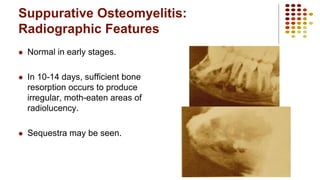
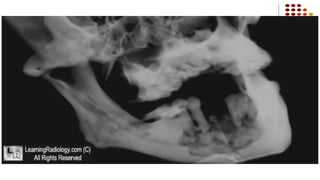
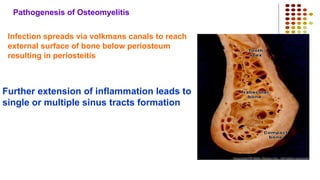

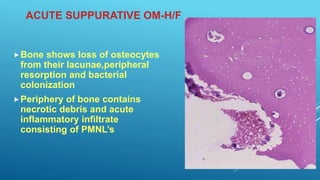
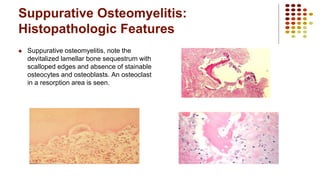
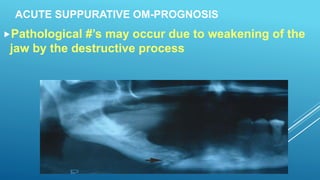
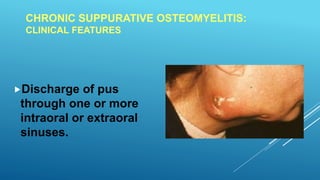



This document discusses osteomyelitis, an inflammation of bone and bone marrow that can result from odontogenic infection. It describes the different types of osteomyelitis including acute suppurative, chronic suppurative, chronic focal sclerosing (condensing osteitis), and chronic diffuse sclerosing osteomyelitis. Specific details are provided on the clinical, radiographic, and histopathologic features of acute suppurative osteomyelitis as well as chronic osteomyelitis with proliferative periostitis (Garre's osteomyelitis). The pathogenesis and potential complications of acute suppurative osteomyelitis are also summarized.































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)


