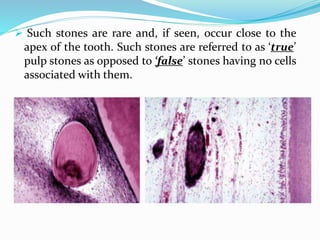
Downloaded 2,003 times

















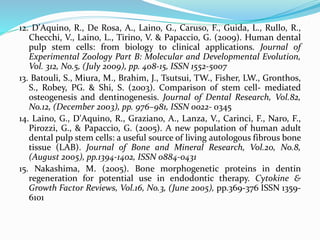
![Some types (of 15) of known collagen
Type Molecular Tissue distribution
Fibril-forming I [a1(I)]2 a2(I) bone, skin, tendon, ligaments
(90%) of body collagen
II [a1(II)]3
cartilage, intervertebral disc,
notochord, vitreous humor of eye
III [a1(III)]3 skin, blood vessels, internal organs
V [a1(V]2 a2(V) as type I
XI [a1(XI] a2(XI) a3(XI) as type II
Fibril-associated IX [a1(IX] a2(IX) a3(IX) cartilage (with type II)
XII [a1(XII)]3 tendon, ligaments (with some type I)
Network-forming IV [a1(IV)]2 a2(IV) basal laminae
VII [a1(VII)]3 anchoring fibrils beneath stratified
squmous epithelia](https://image.slidesharecdn.com/dentalpulp-150226043041-conversion-gate02/85/Dental-pulp-30-320.jpg)































































![References:
1. Seltzer and Bender's Dental Pulp; 2002 by Quintessence Publishing Co, Inc; Rev.
ed. of: The dental pulp / Samuel Seltzer, I.B. Bender. 3rd ed. c1984.
2. Oral histology; Development, Structure and Function: A.R. Ten Cate: 7th Edition
3. Orban’s Oral Histology and Embryology
4. Shafer’s Textbook of Oral Pathology; 5th Edition
5. Yamada, Y., Ito, K., Nakamura, S., Ueda, M. & Nagasaka, T. (2010). Promising cell-
based therapy for bone regeneration using stem cells from deciduous teeth, dental
pulp, and bone marrow. Cell Transplantation. [Epub ahead of print], (October
2010)
6. Gronthos, S., Mangani, M., Brahim, J., Robey, PG. & Shi, S. (2000). Postnatal
human dental pulp stem cells (DPSCs) in vitro and in vivo. Proceedings of the
National Academy of Sciences of the United States of America, Vol.97, No.25,
(December 2000), pp. 13625- 13630, ISSN 0027-8424
7. Miura, M., Gronthos, S., Zhao, M., Lu, B., Fisher, LW., Robey, PG. & Shi, S. (2003).
SHED: stem cells from human exfoliated deciduous teeth. Proceedings of the
National Academy of Sciences of the United Stases of America, Vol.100, No.10,
(May 2003), pp.5807-5812, ISSN 0027-8424](https://image.slidesharecdn.com/dentalpulp-150226043041-conversion-gate02/85/Dental-pulp-109-320.jpg)



The document discusses various aspects of dental pulp, including its structure, functions, and components such as collagens and cells. It emphasizes the vital roles of the dental pulp in supporting tooth vitality, providing nourishment, and acting as a defense against injuries and infections. Furthermore, it addresses the changes in pulp due to aging and the significance of pulp stones in endodontic treatments.













































































