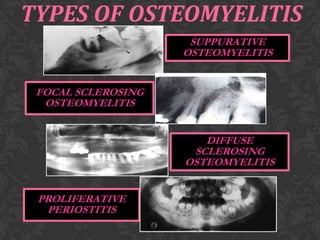
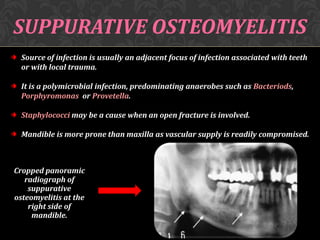
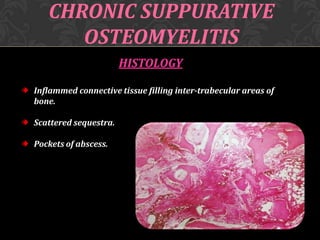
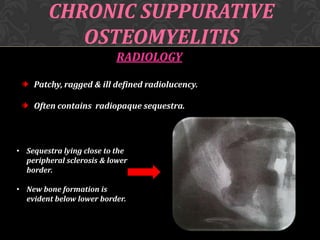
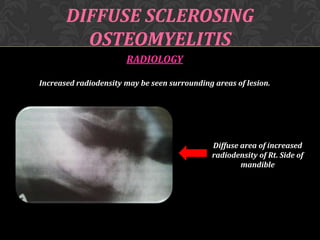
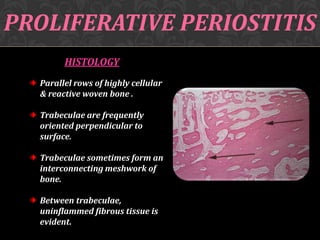
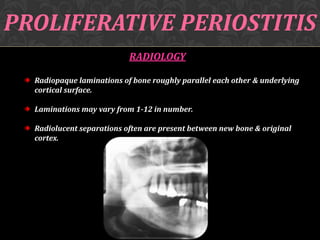
This document discusses osteomyelitis, including its pathogenesis and management. It defines osteomyelitis as an infection of the bone marrow and describes how local and systemic predisposing factors can lead to decreased bone vitality and impaired host defense. The main types of osteomyelitis covered are suppurative, focal sclerosing, diffuse sclerosing, and proliferative perositis. For each type, the document discusses pathogenesis, clinical features, histology, radiology, and management. Key points include how acute suppurative osteomyelitis can progress to chronic form if inadequately treated, and how eliminating infection sources is important but bone changes may persist radiographically for some types.




















































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)


















