Download as PDF, PPTX
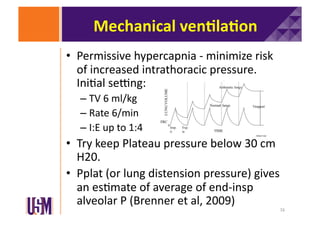
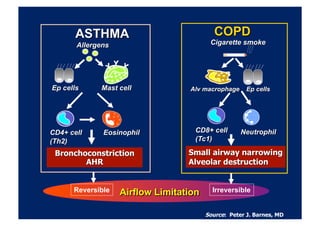

The document discusses updates on asthma and chronic obstructive pulmonary disease (COPD), highlighting key treatments such as continuous nebulization, intravenous beta-2 agonists, and the role of steroids. It emphasizes the importance of recognizing uncontrolled asthma symptoms and the management of COPD through bronchodilators and non-invasive positive pressure ventilation (NIPPV). Additionally, it addresses the controversies surrounding hypoxic drive in COPD and the implications for oxygen therapy in exacerbations.








































































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)
