Downloaded 135 times

































![MANAGING STABLE COPD
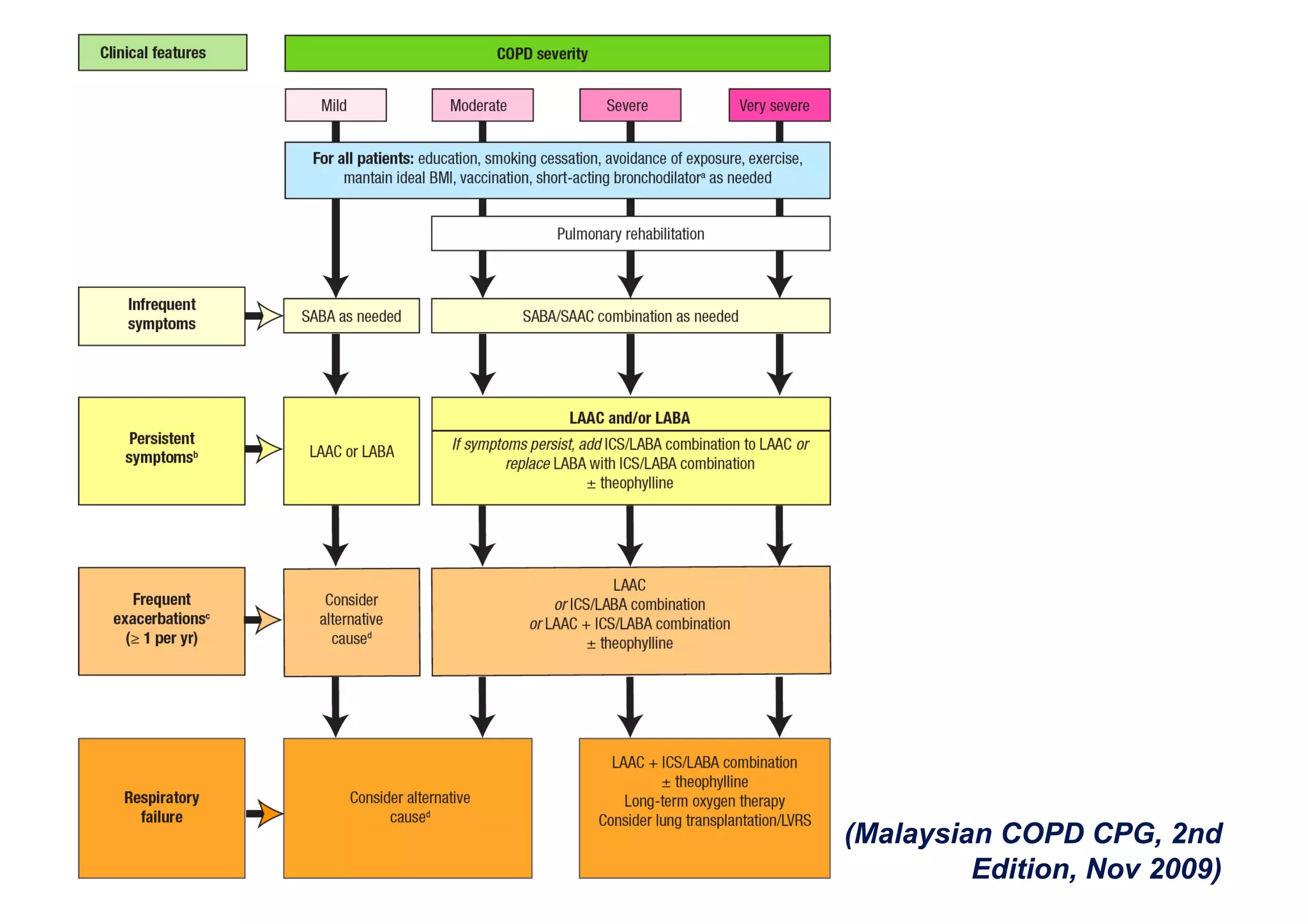
• COPD patients at any stage of disease
severity should be advised to quit smoking
if they still smoke. [Grade A]
• In patients with mild COPD who are
symptomatic, SABA or SAAC or a
combination of both may be prescribed
(Malaysian COPD CPG, 2nd Edition, Nov 2009)](https://image.slidesharecdn.com/copd-100703122025-phpapp02/75/The-2009-COPD-Malaysian-Guidelines-What-s-Important-From-Emergency-Medicine-Perspective-37-2048.jpg)
![MANAGING STABLE COPD
• In patients with moderate to very severe
COPD with persistent symptoms, but
without frequent COPD exacerbations,
either a LAAC or LABA may be initiated.
• If symptoms persist despite this treatment,
an ICS/LABA combination should be
added; and vice versa. [Grade A]
(Malaysian COPD CPG, 2nd Edition, Nov 2009)](https://image.slidesharecdn.com/copd-100703122025-phpapp02/75/The-2009-COPD-Malaysian-Guidelines-What-s-Important-From-Emergency-Medicine-Perspective-38-2048.jpg)












































The document covers the second edition of the Malaysian clinical practice guidelines (CPG) for chronic obstructive pulmonary disease (COPD), emphasizing its definition, pathophysiology, and systemic effects. It highlights the critical role of smoking as a primary risk factor and outlines the management strategies for stable COPD and exacerbations. Lastly, it covers the importance of early diagnosis through spirometry and the need for effective smoking cessation interventions.











![Mechanical ventilation[1]](https://cdn.slidesharecdn.com/ss_thumbnails/mechanicalventilation1-150109002450-conversion-gate01-thumbnail.jpg?width=640&height=640&fit=bounds)































































































