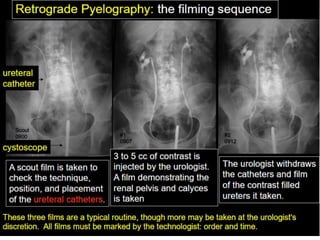
Retrograde pyelography is an x-ray imaging technique used to visualize the kidneys and ureters. A catheter is inserted into the ureter and contrast dye is injected under fluoroscopy. Images are taken of the renal pelvis, ureters and bladder. It is used to evaluate abnormalities seen on intravenous urograms or investigate causes of hematuria when the ureters were not fully visualized. The procedure has some risks but is less risky than intravenous urography. It can demonstrate various conditions like ureteral strictures, filling defects, diverticula or stenosis. Care is taken during injection to avoid overdistension and complications.