Downloaded 625 times







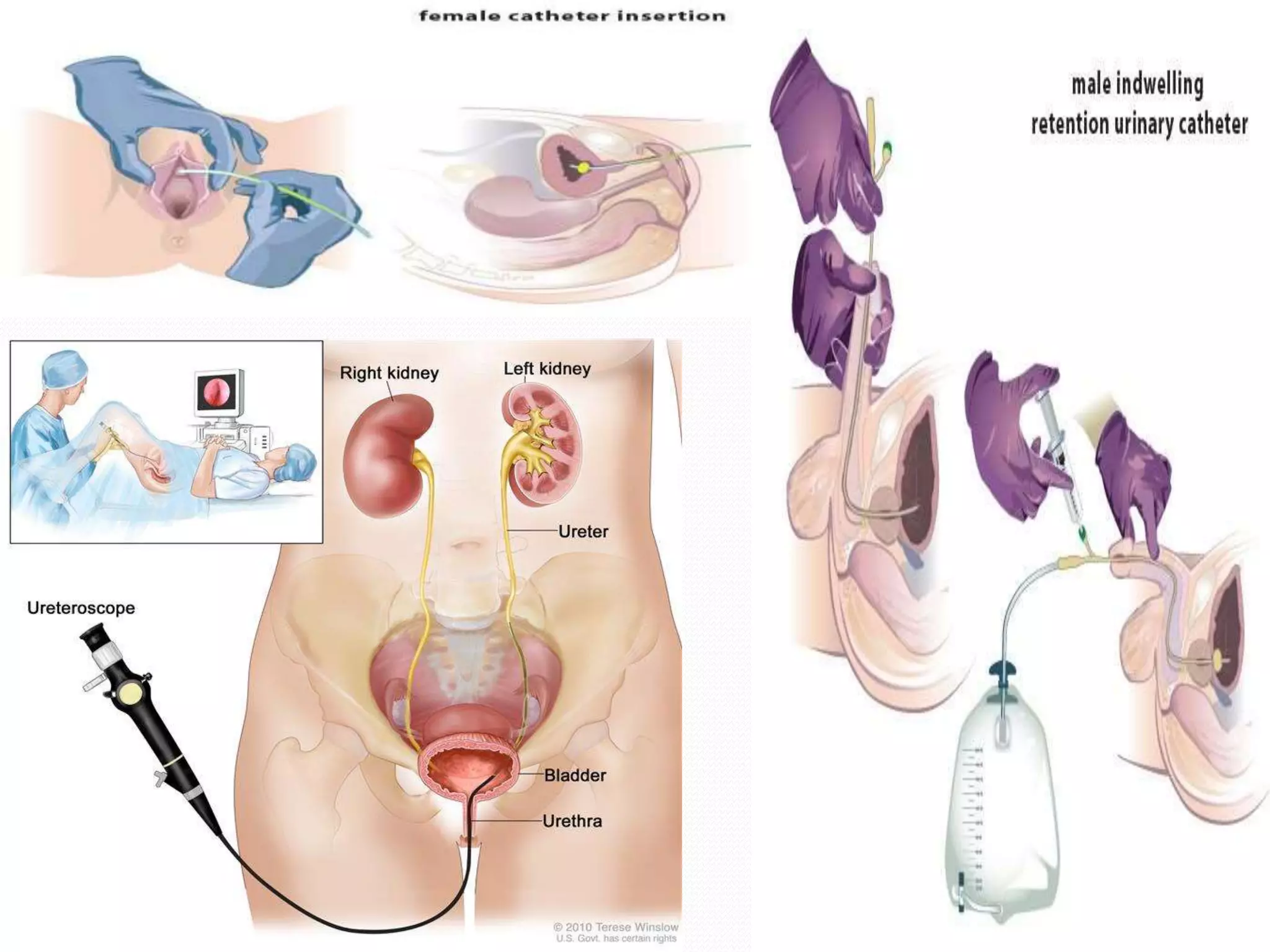






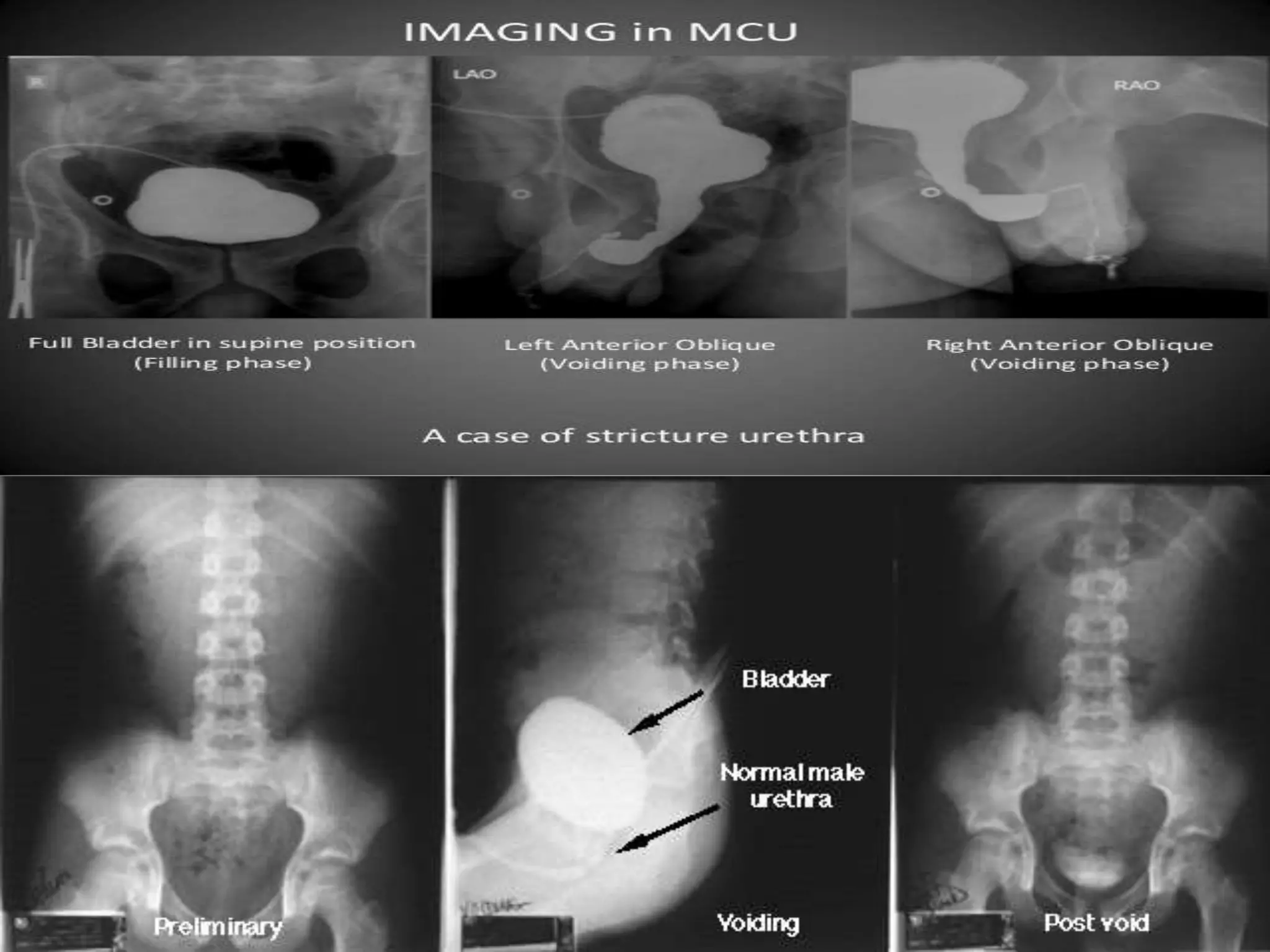




This document provides information on retrograde urethrography (RGU), ascending urethrogram (ASU), and micturating cystourethrography (MCU). RGU and ASU involve injecting iodinated contrast media through the urethra under fluoroscopy to image the urethra. MCU images the lower urinary tract by introducing contrast into the bladder via catheter and having the patient void to detect reflux or other issues. The document outlines indications, contraindications, equipment, techniques, imaging views, and potential complications for each procedure.