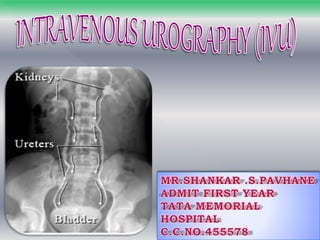
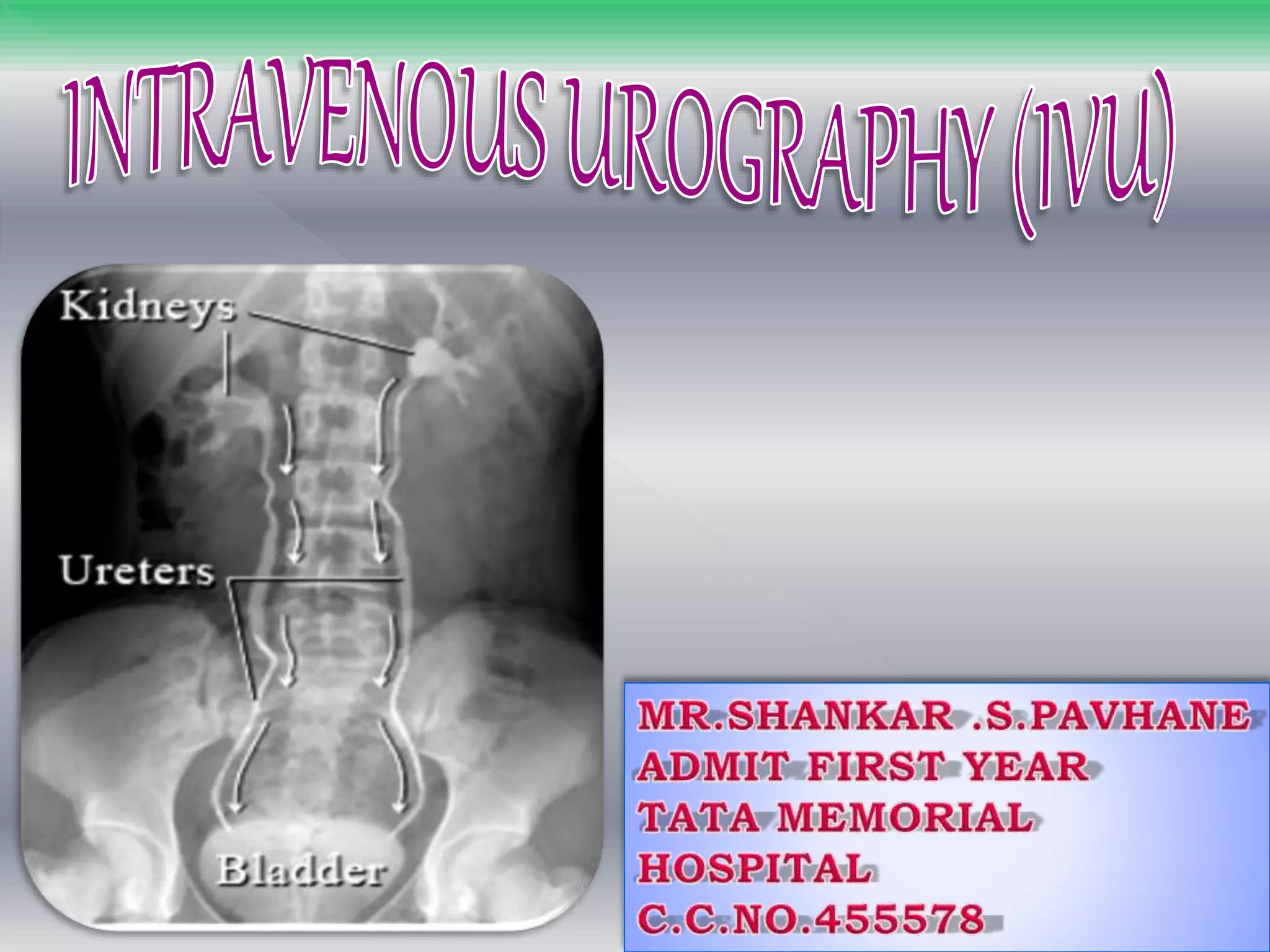
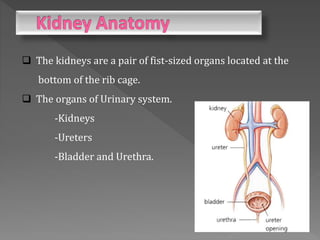
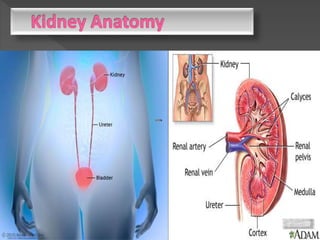
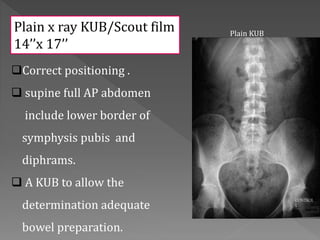
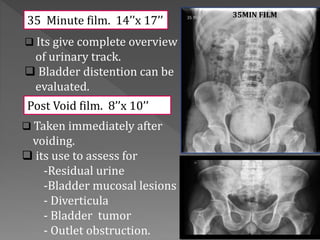
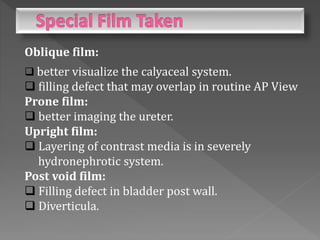
Intravenous urography (IVU) is a radiographic procedure used to evaluate the urinary system, administered after an intravenous contrast media injection. It is employed for diagnosing conditions such as obstructive uropathies, congenital anomalies, and renal pathologies while requiring careful patient assessment including history and preparation. Various imaging techniques and positioning are outlined to ensure accurate evaluation of the renal system, including the use of compression and different film types.





















































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)


