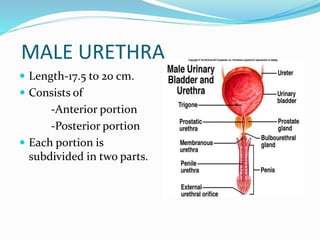
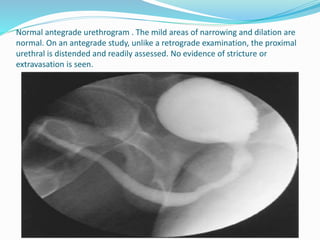
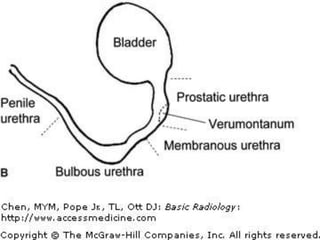
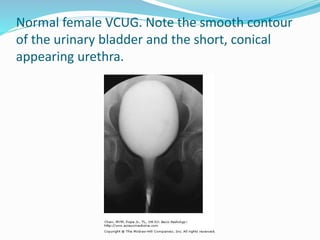
The document describes the anatomy and radiographic evaluation of the urethra. It discusses the male and female urethra anatomy in detail. Retrograde urethrography and voiding cystourethrography are described as the main modalities for urethral imaging. Retrograde urethrography is used to evaluate traumatic injuries, strictures, and fistulas in men. Voiding cystourethrography is useful to assess the urethra during micturition and to detect vesicoureteric reflux in children.