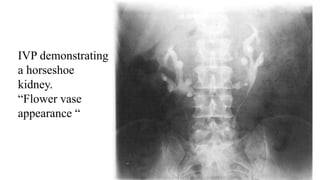
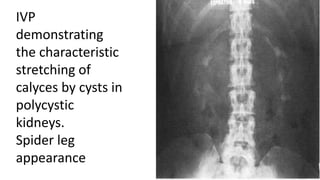
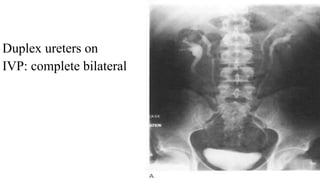
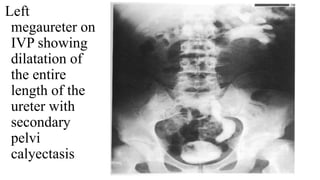
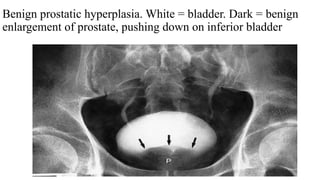
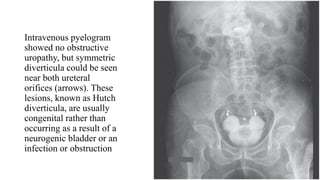
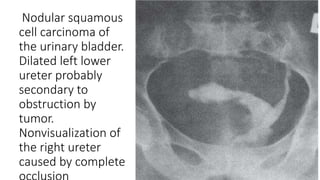
The document describes a case presentation of a 10-year-old male child who presented with abdominal pain. An ultrasound and intravenous pyelogram (IVP) were performed. The ultrasound found right pyonephrosis, right and left renal calculi, and left hydroureteronephrosis. The IVP confirmed these findings and also found a right ureteric calculus and question of a left ureteric stricture. The document then provides details on IVP, including how it is performed, indications, advantages, limitations, normal findings, and examples of various abnormalities that can be seen on an IVP.