Downloaded 1,727 times
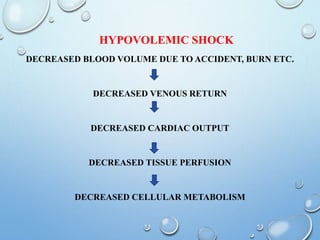
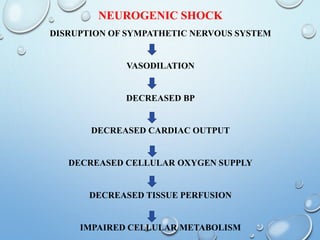
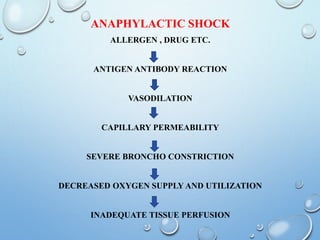
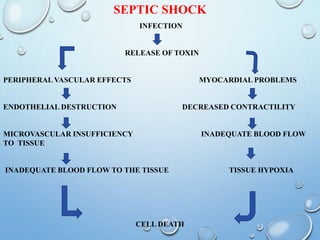
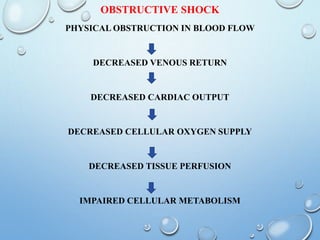


The document provides a comprehensive overview of shock in medical surgical nursing, defining it as a condition where tissues do not receive enough oxygen and nutrients. It classifies shock into five types: cardiogenic, hypovolemic, obstructive, and distributive (including neurogenic, anaphylactic, and septic), and outlines their causes, pathophysiology, clinical manifestations, diagnostics, and management strategies. Management includes both medical and surgical approaches, along with detailed nursing assessments and interventions.






















































































