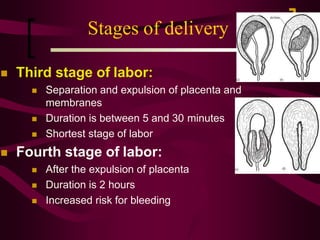
Normal labor is defined as the contractions of the uterus that result in the expulsion of the fetus between 37 and 42 weeks of gestation, characterized by spontaneous delivery without complications. The document outlines the stages of labor, including descriptions of cervical changes, contractions, and the overall process from dilation to delivery of the placenta. Factors affecting labor progression are discussed, along with fetal positions and presentations during the birthing process.




































































































![Normal labour [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/normallabourautosaved-200123025541-thumbnail.jpg?width=640&height=640&fit=bounds)












































