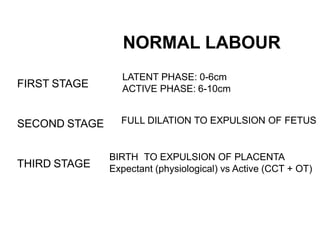
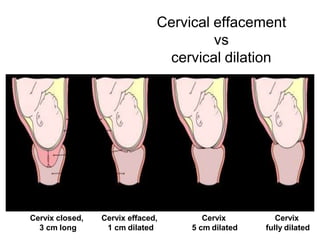
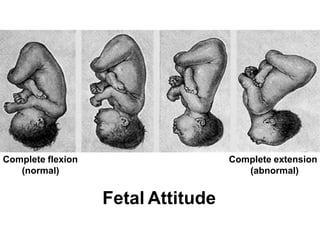
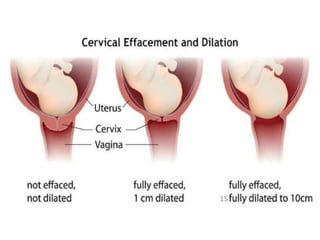
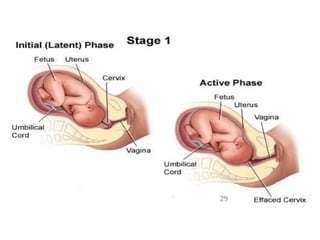
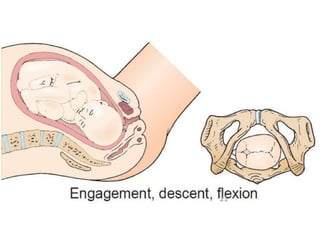
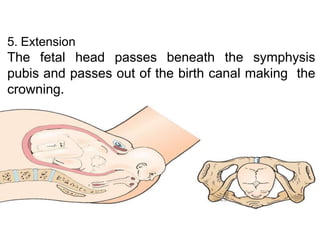
This document provides an outline on normal labor and the mechanism of labor. It defines labor as the physiological process of expelling the fetus, placenta, and membranes through the birth canal after 24 weeks of pregnancy. Normal labor fulfills criteria of spontaneous onset at term, vertex presentation, no prolongation, and natural termination with minimal aids. The document describes the three stages of labor as well as the cervical changes, fetal positioning, and mechanisms involved in labor including engagement, descent, flexion, rotations, and expulsion of the fetus through the birth canal. It emphasizes the importance of classifying pregnancies as high or low risk and addressing any medical issues to ensure a safe delivery.