




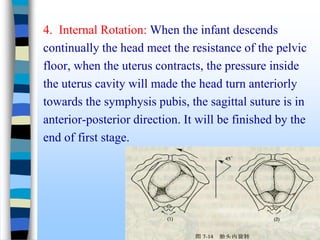
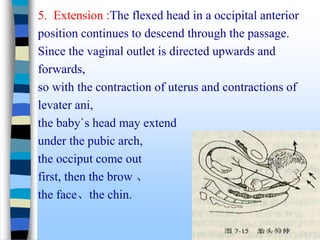
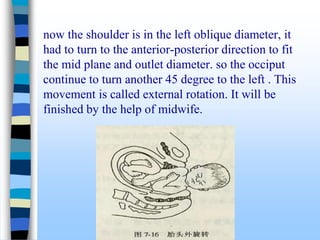
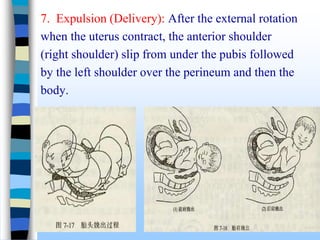

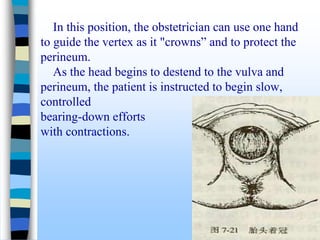
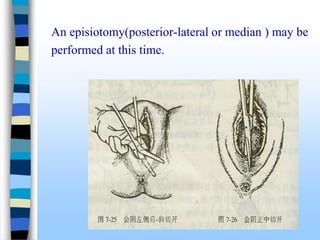


The document describes the normal mechanism of labor, including the three stages of labor and the fetus' seven passive movements that enable it to navigate the birth canal. The first stage involves cervical dilation. The second stage is when the fetus is delivered. The third stage involves delivery of the placenta. Key movements include engagement, descent, flexion, internal rotation, extension, restitution/external rotation, and expulsion. Close monitoring of the fetus and mother is important throughout labor.



































![mechanism_of_labor[1].pptx obstetrics and gynaecology midwifery nursing mater...](https://cdn.slidesharecdn.com/ss_thumbnails/mechanismoflabor1-250610164745-6b6dfb9d-thumbnail.jpg?width=640&height=640&fit=bounds)



















































