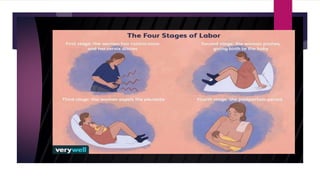
Normal labor involves a series of events that lead to the expulsion of the fetus, placenta, and membranes from the uterus through the vagina. It is divided into three stages: first stage involves cervical dilation, second stage involves fetal descent and expulsion, and third stage involves placental delivery. The document outlines the cardinal movements that make up the mechanism of labor, including engagement, descent, flexion, internal rotation, crowning, extension, restitution, and external rotation to facilitate the fetus' passage through the birth canal.


![NORMAL LABOR
[EUTOCIA]
Labor is called normal if it fullfils the following criteria;
• Spontaneous in onset and at term
• With vertex presentation
• Without undue prolongation
• Natural termination with minimal aids
• Without having any complications affecting the health of
mother and/ Or the baby.](https://image.slidesharecdn.com/normallabor1-231023111431-10ae4d81/85/Normal-labor-1-pptx-4-320.jpg)