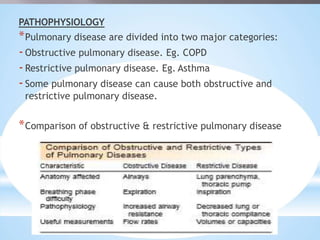
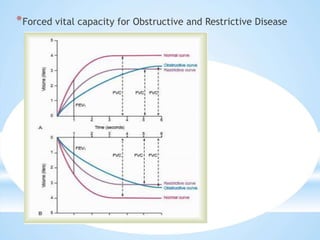
Pulmonary function tests (PFT) are critical procedures to evaluate lung function, categorize pulmonary diseases, and assess therapeutic effectiveness. They include dynamic and static tests, with spirometry being a key method for measuring airway function and capacity. Proper administration and interpretation of PFTs are essential in diagnosing respiratory diseases and preparing patients for surgery.