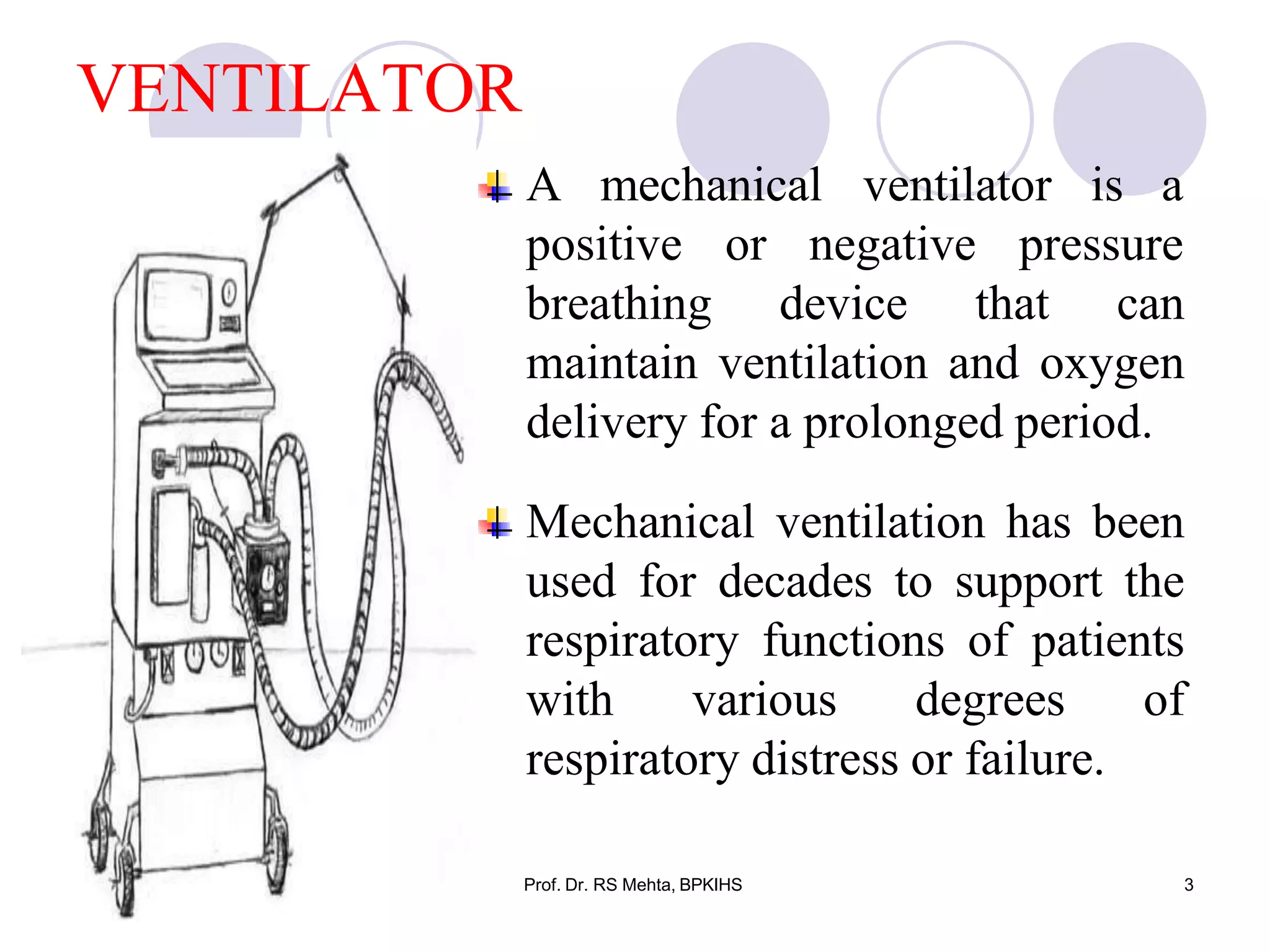
The document discusses mechanical ventilation and various ventilator modes. It begins by defining mechanical ventilation as a breathing device that can maintain oxygen delivery through positive or negative pressure. It then describes the purposes and indications for mechanical ventilation. The main classifications of ventilators are described as negative pressure ventilators, which use suction, and positive pressure ventilators, which provide airflow into the lungs. Important ventilation modes like CPAP, PEEP, and SIMV are also summarized.




























































































































![Simulation_lecture_11_mechanical_ventillation[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/simulationlecture11mechanicalventillation1-240330192829-1f83f7bc-thumbnail.jpg?width=640&height=640&fit=bounds)