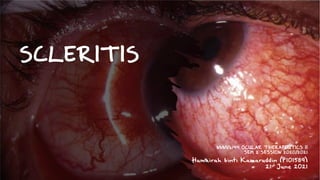
Scleritis (Inflammation of Sclera)
•
1 like•58 views

It is about scleritis. I try make it simple and sweet during my studies. Hope it would be beneficial for you too!

Recommended
More Related Content
What's hot
Similar to Scleritis (Inflammation of Sclera)
Similar to Scleritis (Inflammation of Sclera) (20)
Recently uploaded
Recently uploaded (20)
Scleritis (Inflammation of Sclera)
- 1. SCLERITIS NNNV6144 OCULAR THERAPEUTICS II SEM 2 SESSION 2020/2021 Humairah binti Kamaruddin (P101589) 21st June 2021
- 2. SCLERITIS Anterior Posterior (6%) Diffuse (75%) Nodular (14%) Necrotizing (5%) With inflammation (4%) • Vaso-occlusive necrotizing scleritis • Granulomatous necrotizing scleritis • Surgically induced necrotising scleritis (SINS) Without inflammation (1%) • Scleromalacia perforans Sainz de la Maza, M., Molina, N., Gonzalez-Gonzalez, L. A., Doctor, P. P., Tauber, J., & Foster, C. S. (2012). Clinical characteristics of a large cohort of patients with scleritis and episcleritis. Ophthalmology, 119(1), 43–50. https://doi.org/10.1016/j.ophtha.2011.07.013
- 3. SYMPTOMS • Severe & boring eye pain – awake at night • Worsen with eye movement, with touch. • May radiate ipsilateral to face, cheek & jaw. • Gradual/acute onset red eye. • Tearing, photophobia, decrease in vision. • Recurrent episode is common.
- 4. • Deep episcleral plexus dilated • Tender & immobile nodule • Bluish violaceous hue (observed in natural light) • Scleral vessels do not blanch vs episcleritis (on application of topical phenylephrine 2.5%) • Local/ diffuse violaceous nodular • Thin, bluish sclera SIGNS • Scleral edema, intense hyperemia • Necrotic/avascular plaques surrounded by mildly dilated episcleral vessels. !!! Before drop phenylephrine, test for tenderness with cotton bud.
- 5. Slit-beam view nodular Episcleritis vs. Scleritis A slit lamp section shows an underlying flat anterior scleral surface, indicating the absence of scleritis. Deep beam is not displaced above the scleral surface Slit illumination shows superficial displacement of the entire beam
- 6. ETIOLOGY • Infectious (i.e Herpes zoster, Syphilis, Tuberculosis) • Post surgery (i.e scleral buckling, pterygium surgery) • Trauma (i.e penetrating injury contaminated by soil or vegetable) • Rheumatoid arthritis (RA) • Granulomatosis with polyangiitis (GPA) • Relapsing polychondritis (RP) • Polyarteritis nodosa (PAN) • Systemic lupus erythematosus (SLE) • Ankylosing spondylitis (AS) • Inflammatory bowel disease (IBD) • Associated systemic disease:
- 7. INVESTIGATION • B-scan: T-sign (suggestive of posterior scleritis) • Complete blood count (CBC) • ESR/CRP • Serological tests: o Rheumatoid factor (R.A factor) o ANA (antinuclear antibodies) o Anti ds DNA antibody o ANCA (antineutrophil cytoplasmic antibodies) o VDRL, FTA-ABS Hyporeflectivity from optic nerve and fluid under Tenon’s capsule • Fundus angiography • OCT • Urine sediment • Chest X-ray • Tuberculin skin tests
- 8. POTENTIAL COMPLICATION • Scleral melt • Corneal melt • Anterior uveitis • Cataract • Glaucoma • Exudative retinal detachment • Staphyloma
- 9. TREATMENT • Systemic treatment: • Adequate control of the underlying condition. • Oral NSAID • Oral Prednisolone • Intravenous methylprednisolone • Immunosuppressive therapy • Surgical treatment: • Scleral grafting • Biologic immunomodulatory agents • Alkylating agents • Scleral debridement • Systemic (& topical) antimicrobials Infectious scleritis !!! Can start steroid as well to control inflammation !!! Sclera to sclera grafting is hard. Common use amniotic membrane grafting.
- 10. PROGNOSIS • Nonnecrotizing noninfectious anterior (diffuse or nodular) scleritis : • Necrotizing scleritis, posterior scleritis or infectious scleritis : Good prognosis with treatment High risk of permanent vision loss At risk of higher mortality rates
- 11. Diffuse anterior scleritis / diffuse non-necrotizing anterior scleritis Nodular anterior scleritis / nodular non-necrotizing anterior scleritis Vaso-occlusive necrotizing anterior scleritis Granulomatous necrotizing scleritis SINS following trabeculectomy Patient with rheumatoid arthritis. Asymptomatic necrotic patch Moderate Severe thinning and exposure of uvea Necrotizing anterior scleritis without inflammation (Scleromalacia perforans) Necrotizing anterior scleritis with inflammation
- 12. REFERENCES • 2019-2020 BCSC (Basic and Clinical Science Course), Section 09: Uveitis and Ocular Inflammation (MAJOR REVISION) • 2016. The Wills Eye Manual. 7th ed. Philadelphia, PA: Lippincott Williams and Wilkins.