

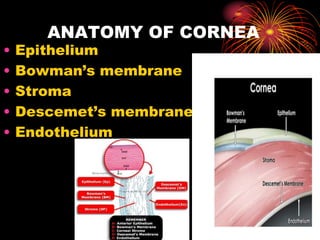

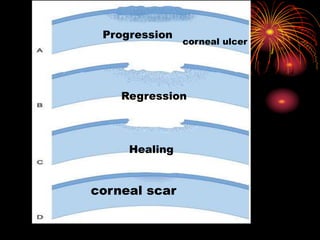
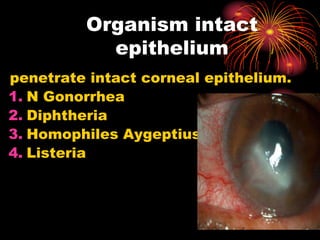
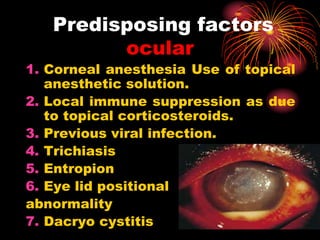





















This document provides an overview of corneal diseases and anatomy. It discusses the layers of the cornea, its nerve supply, functions, and normal defense mechanisms. Major sections cover diseases like keratitis, degeneration, ectasies, and congenital anomalies. Specific diseases covered in detail include bacterial, fungal, viral, and mechanical keratitis. Predisposing factors, symptoms, signs, treatment, and complications are described for various corneal diseases including hypopyon ulcer, fungal ulcer, herpes simplex keratitis, and varicella zoster viral keratitis. Degenerations like arcus senilis and band keratopathy are also summarized.




























































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)


















