Download as PDF, PPTX
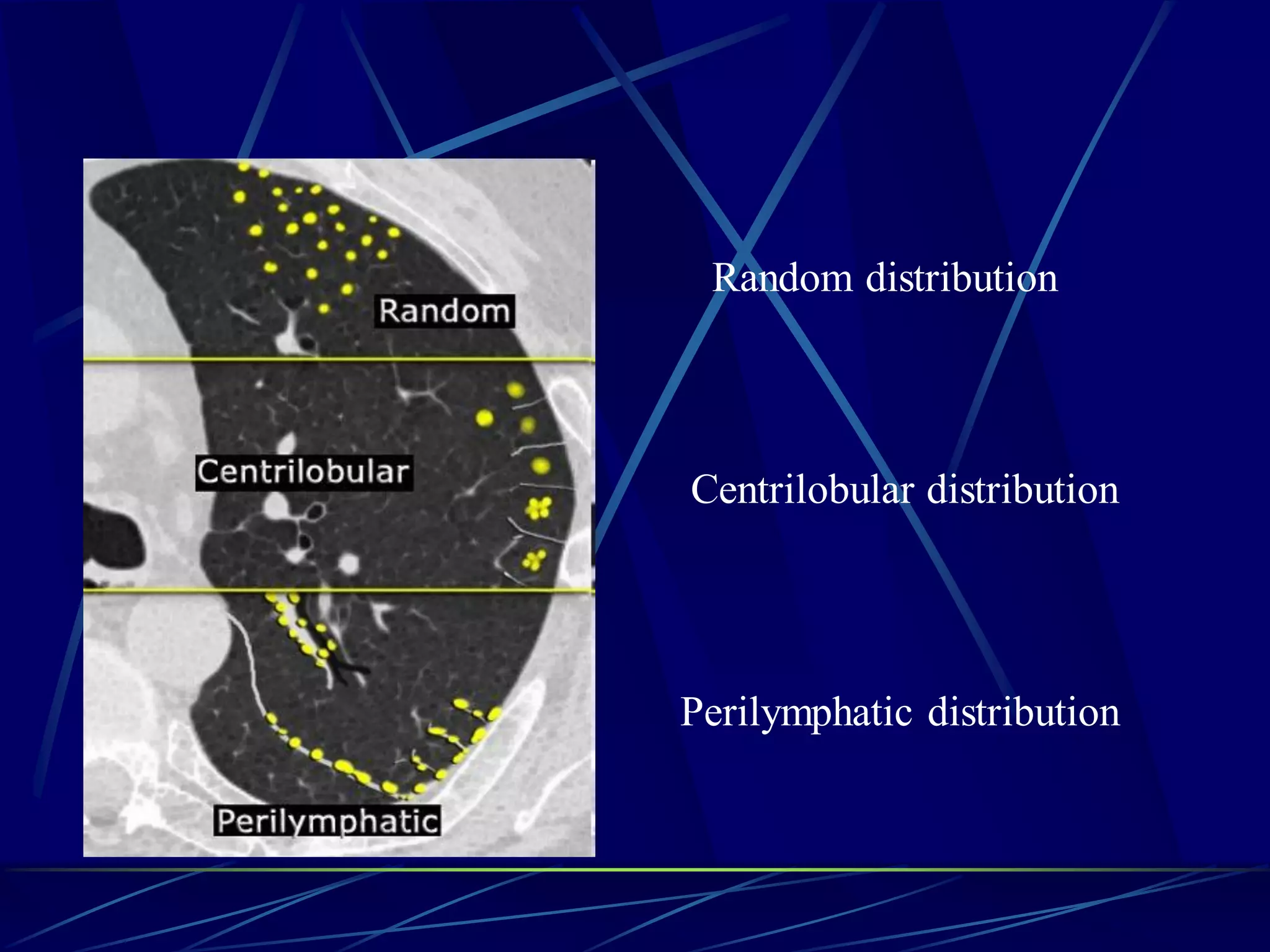
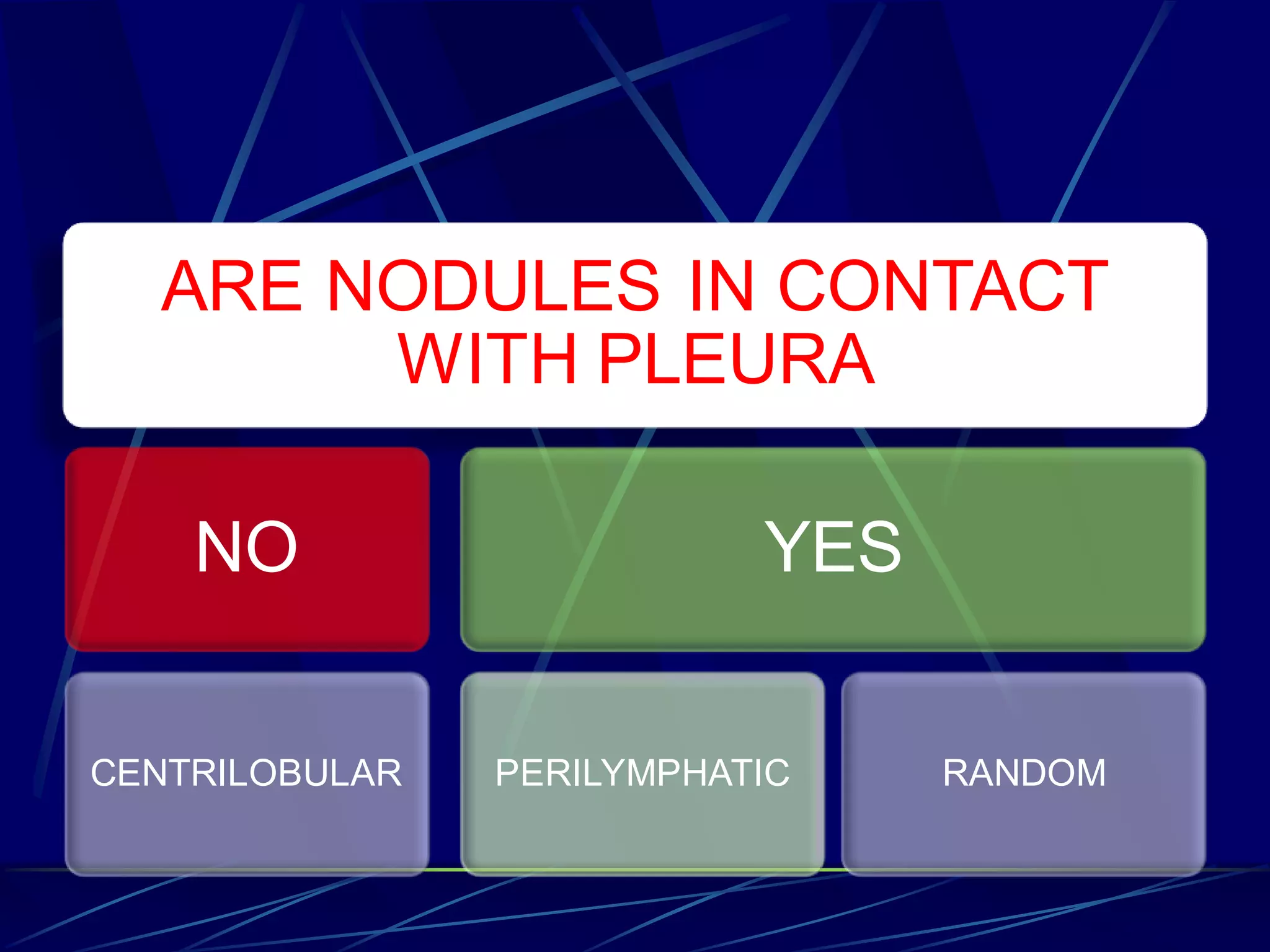
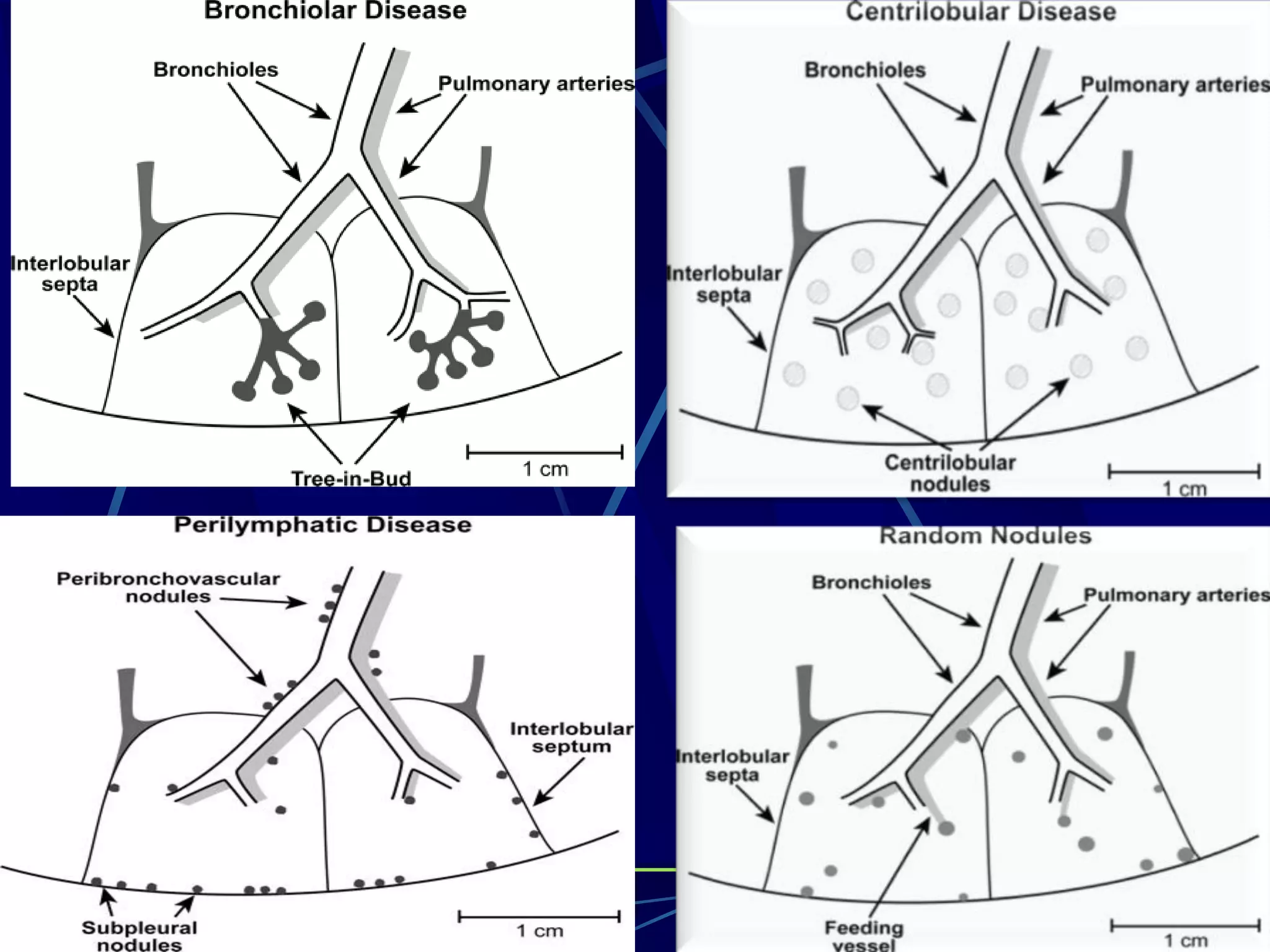
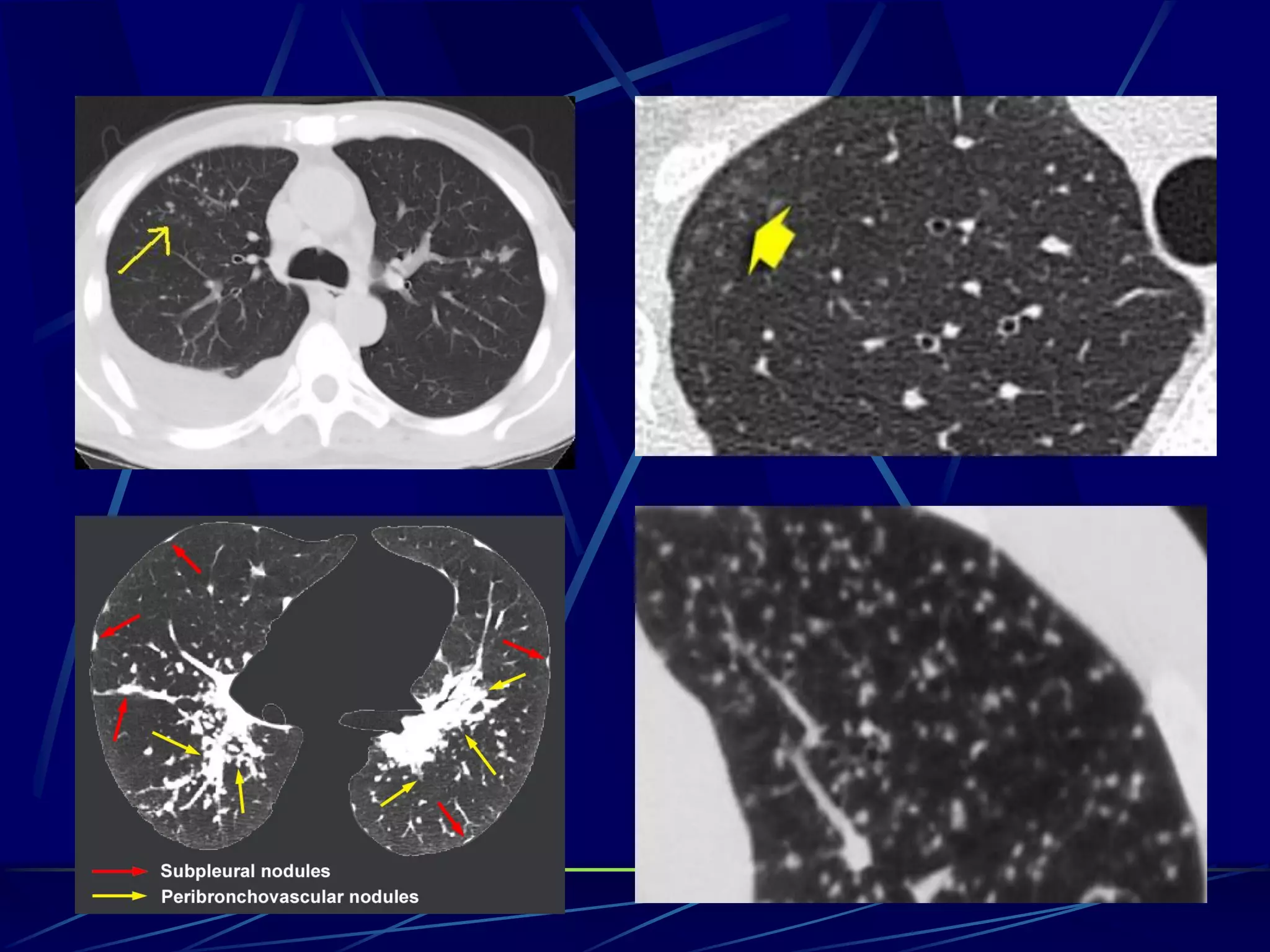
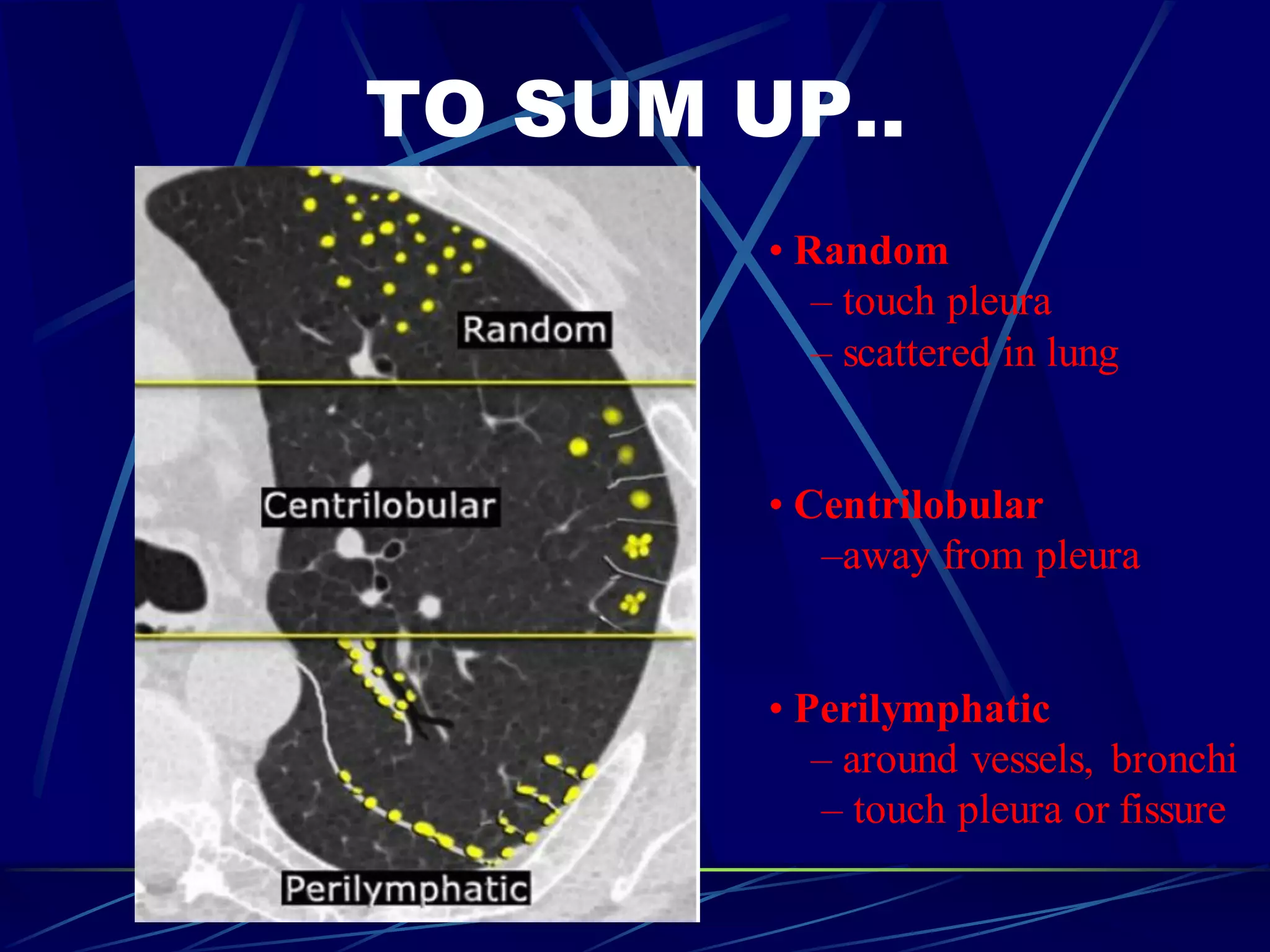
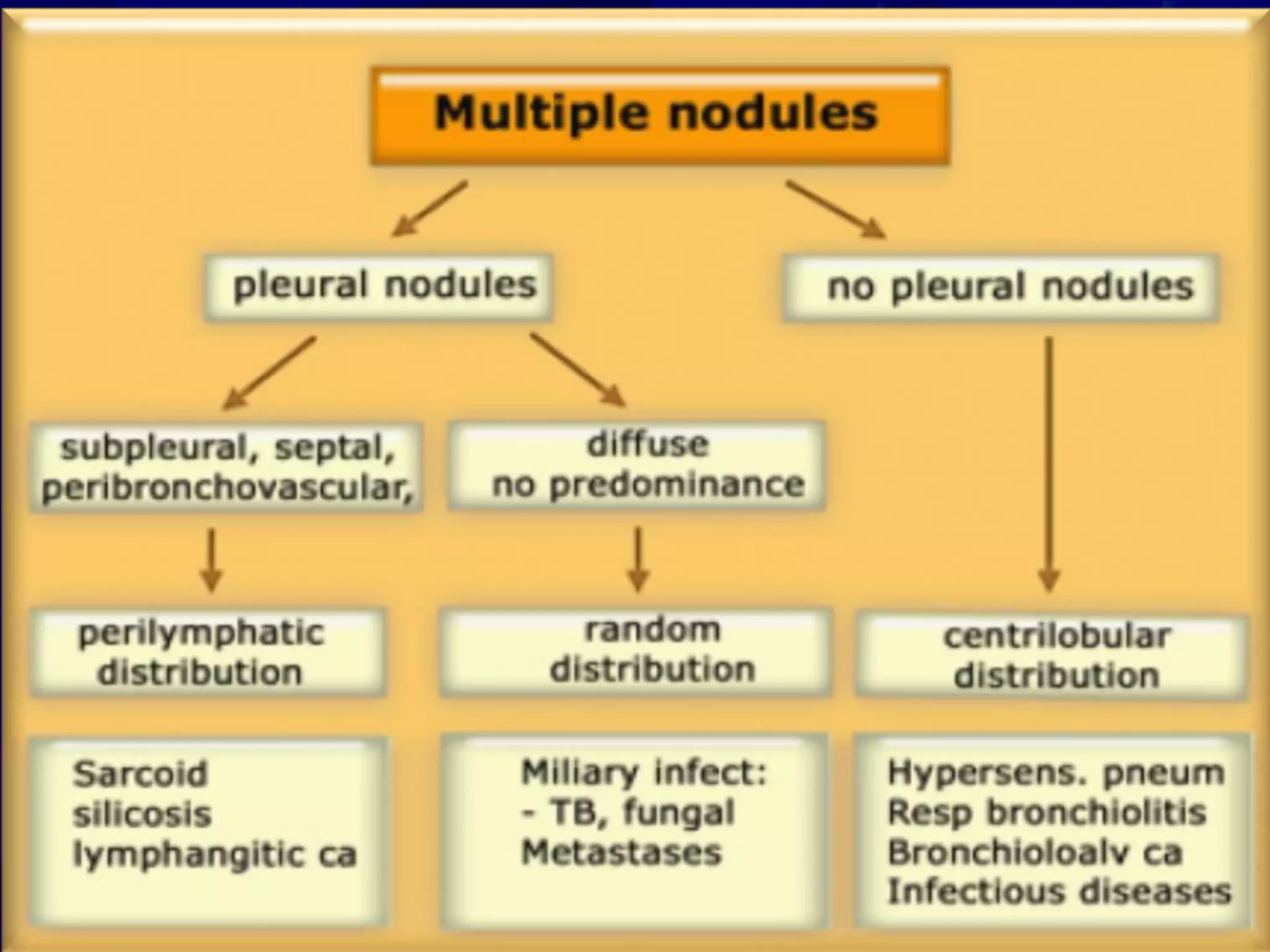
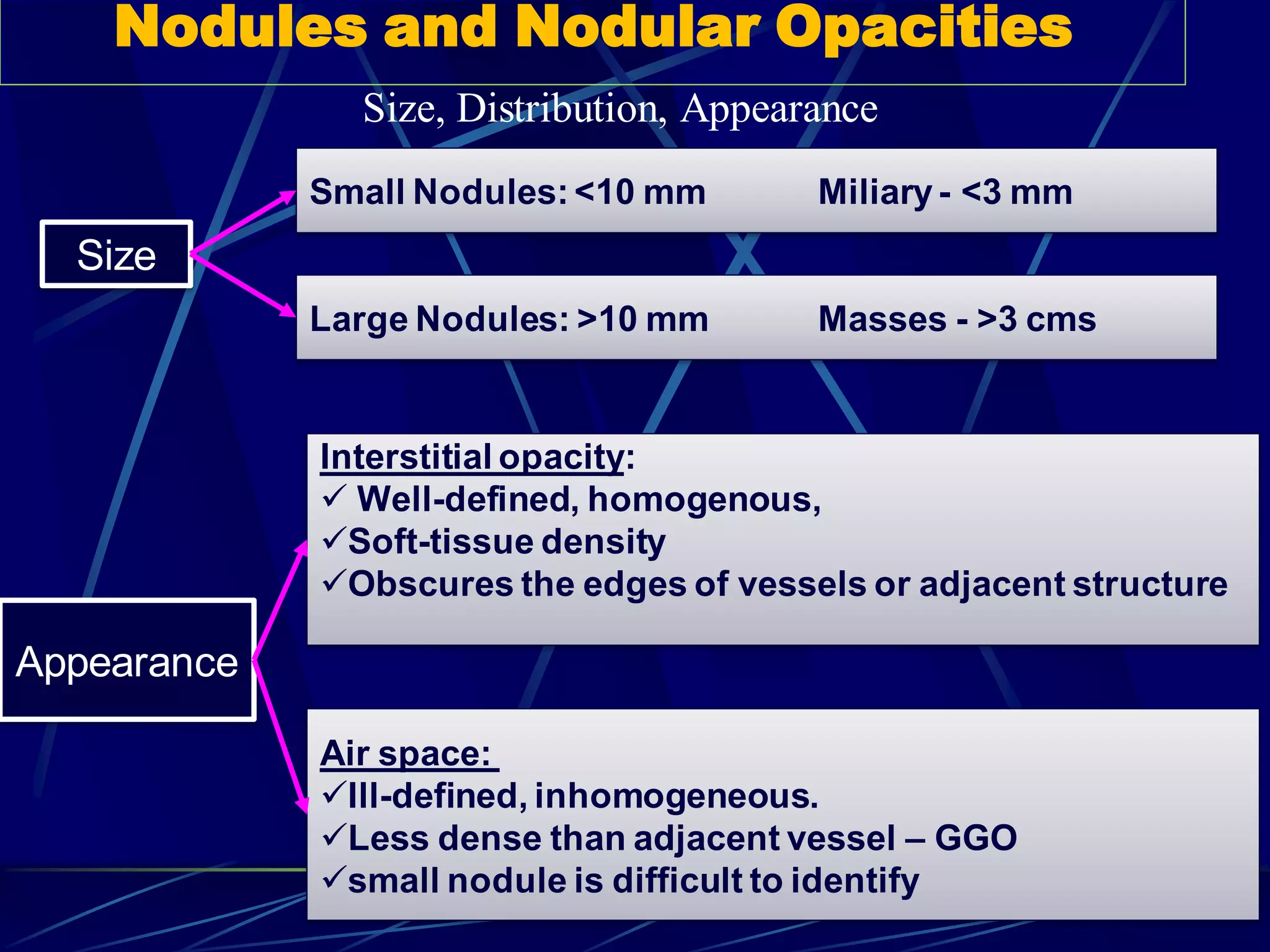
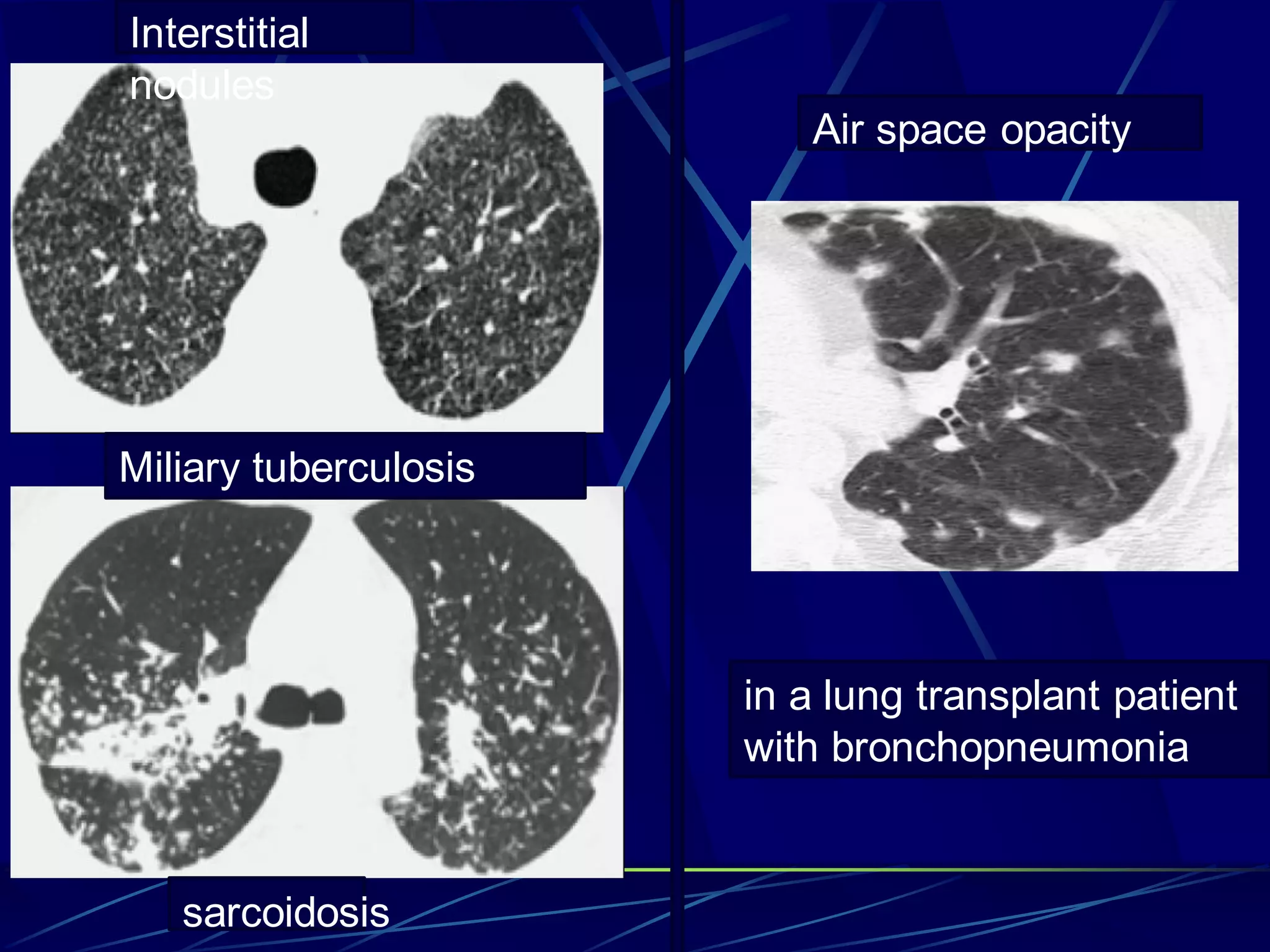
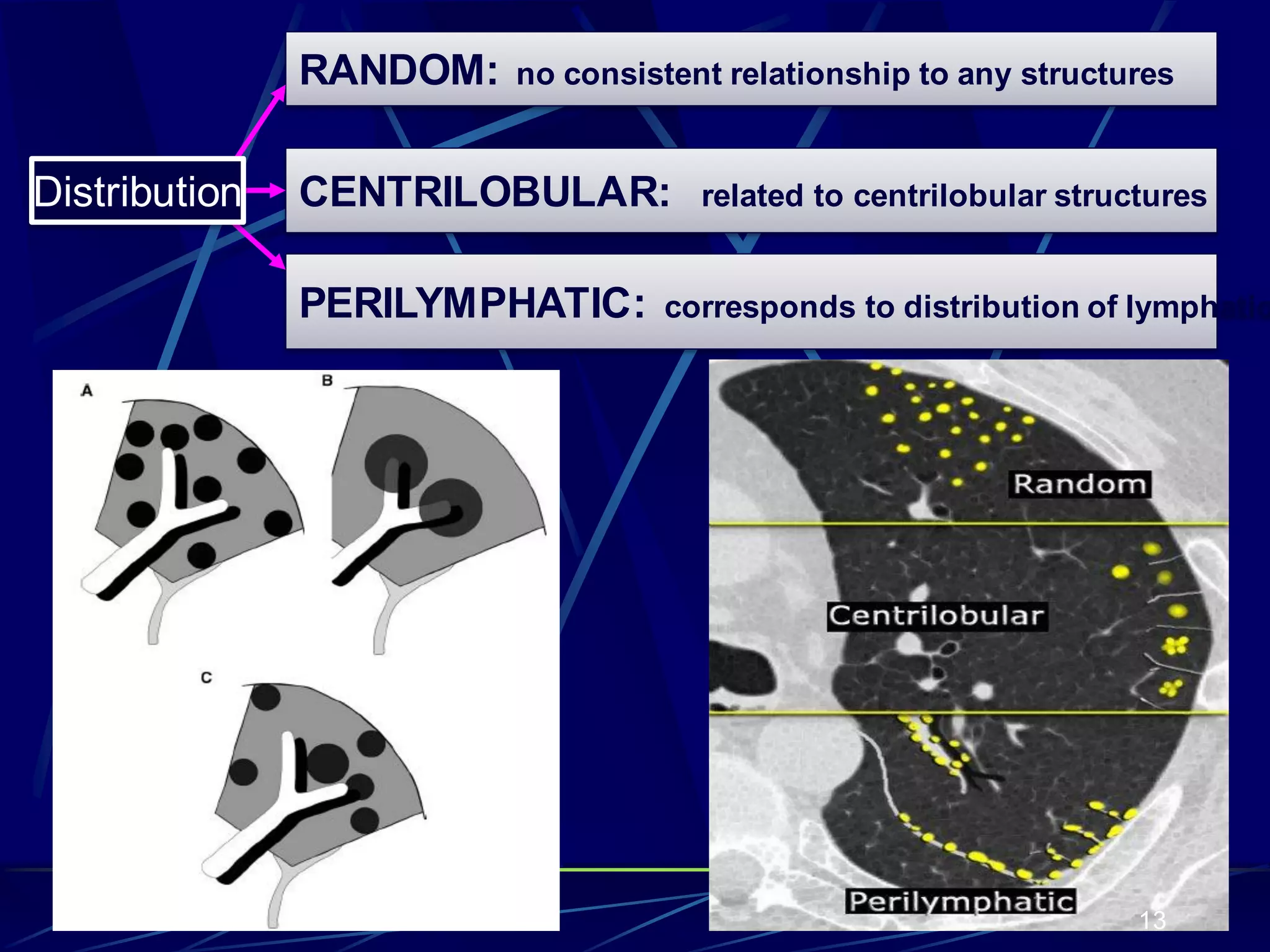
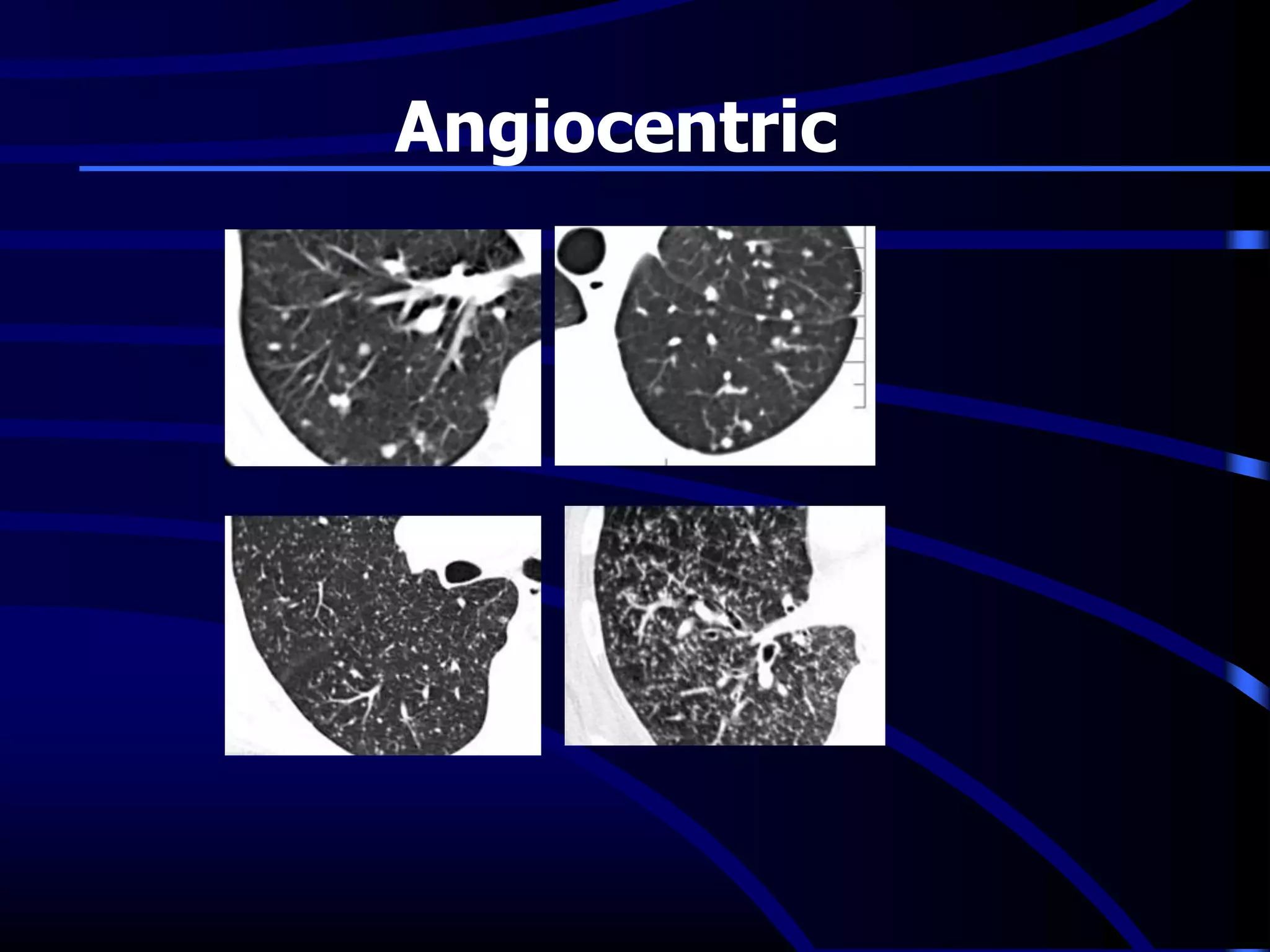
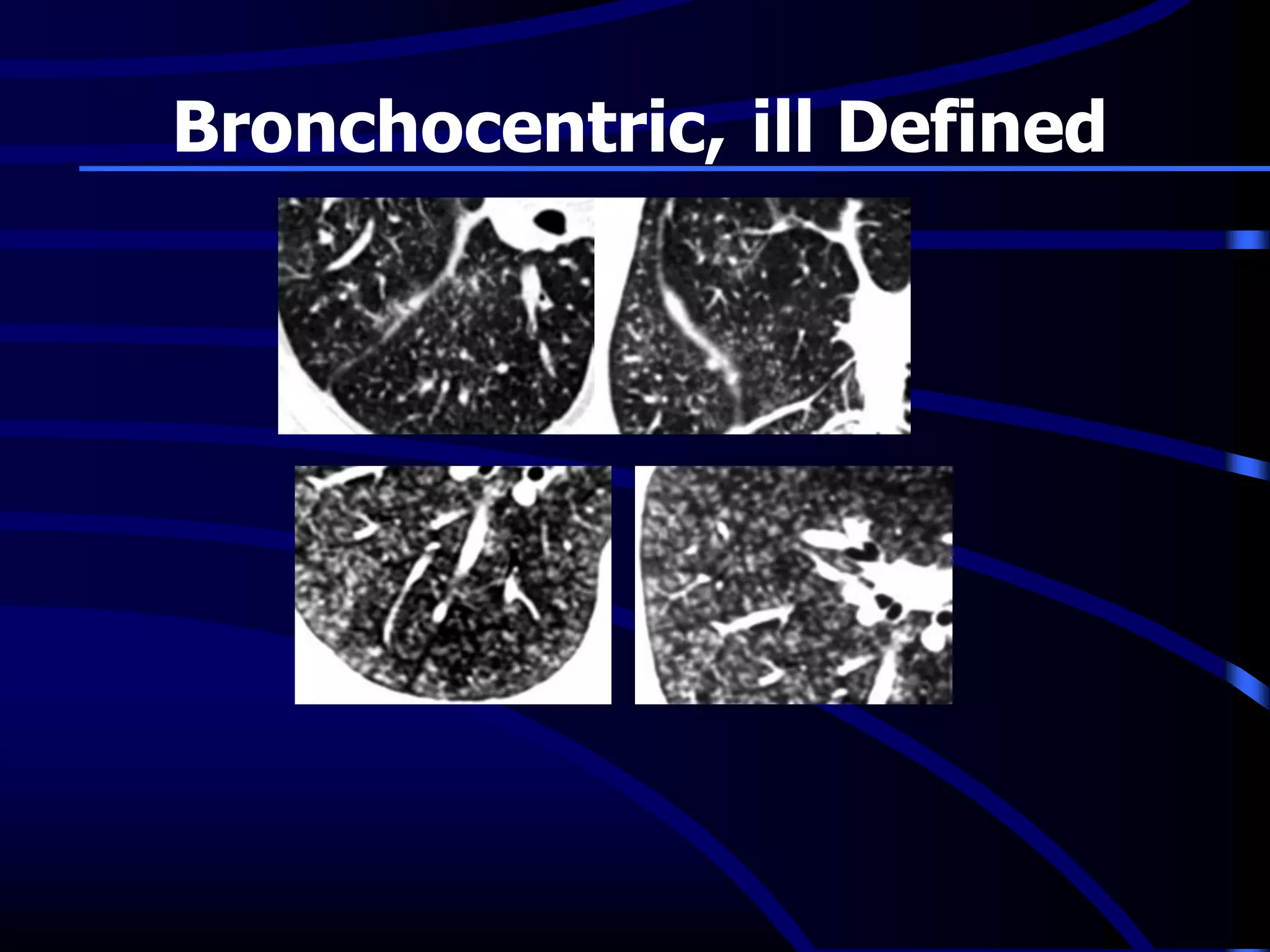
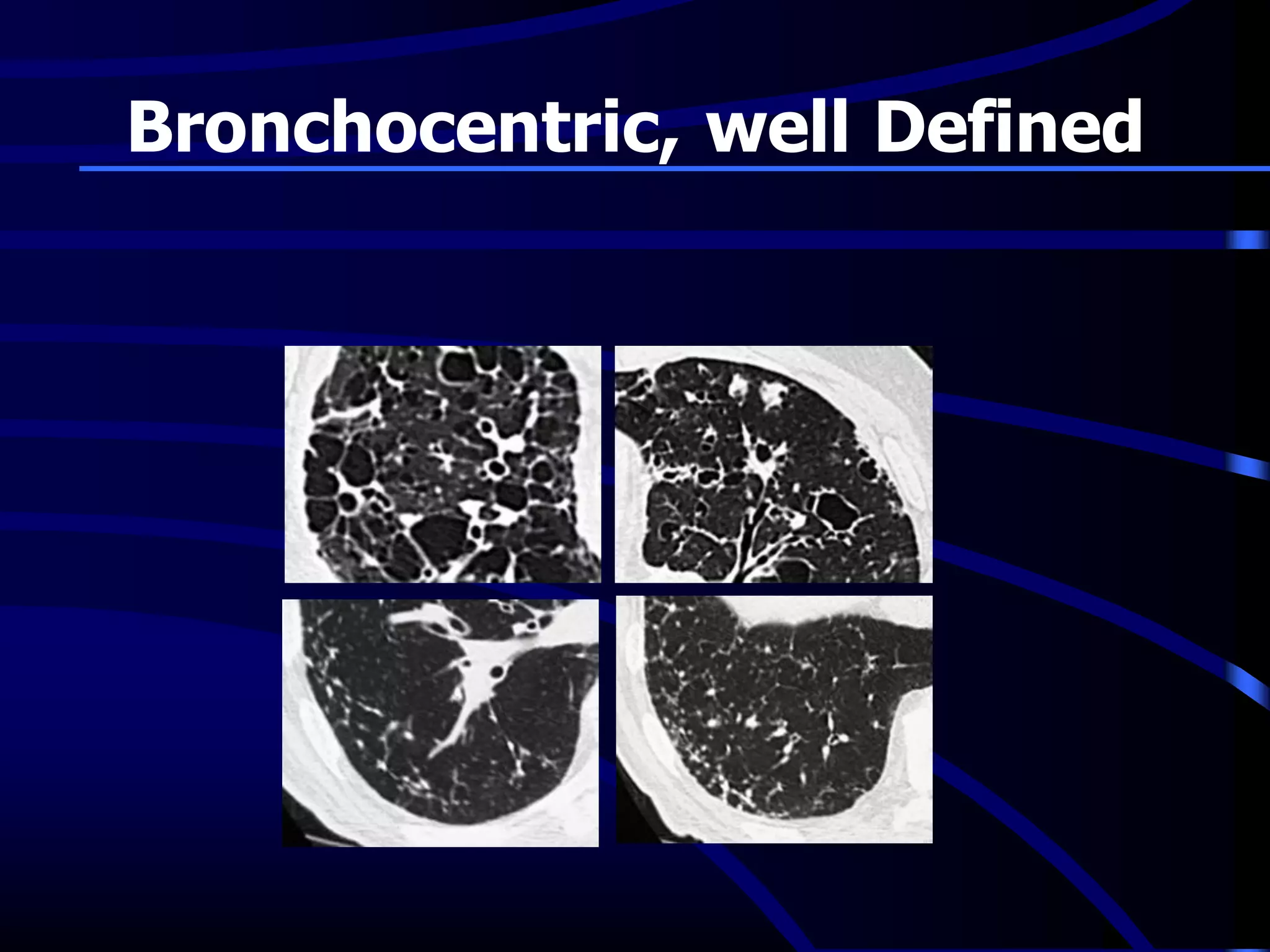
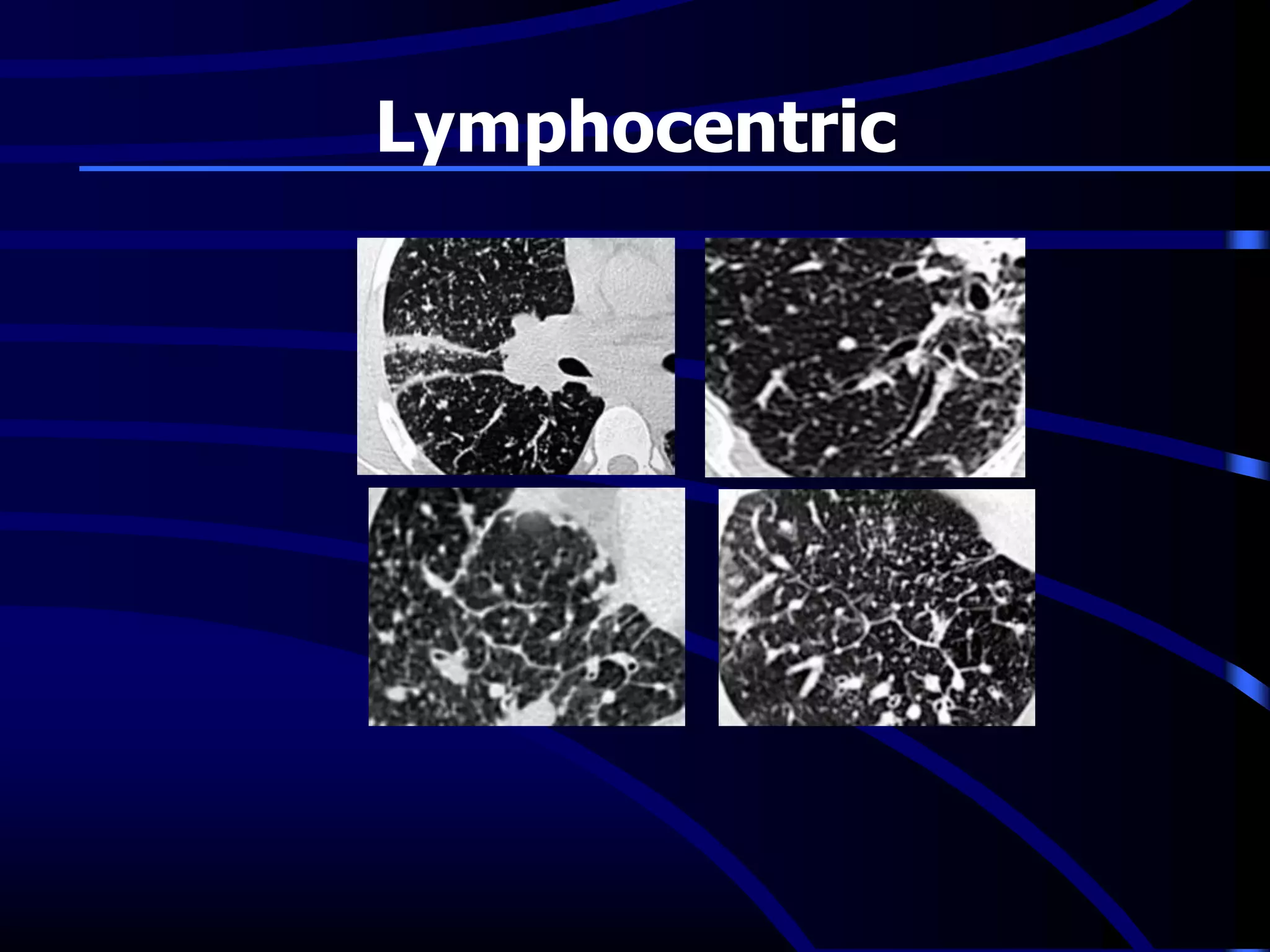
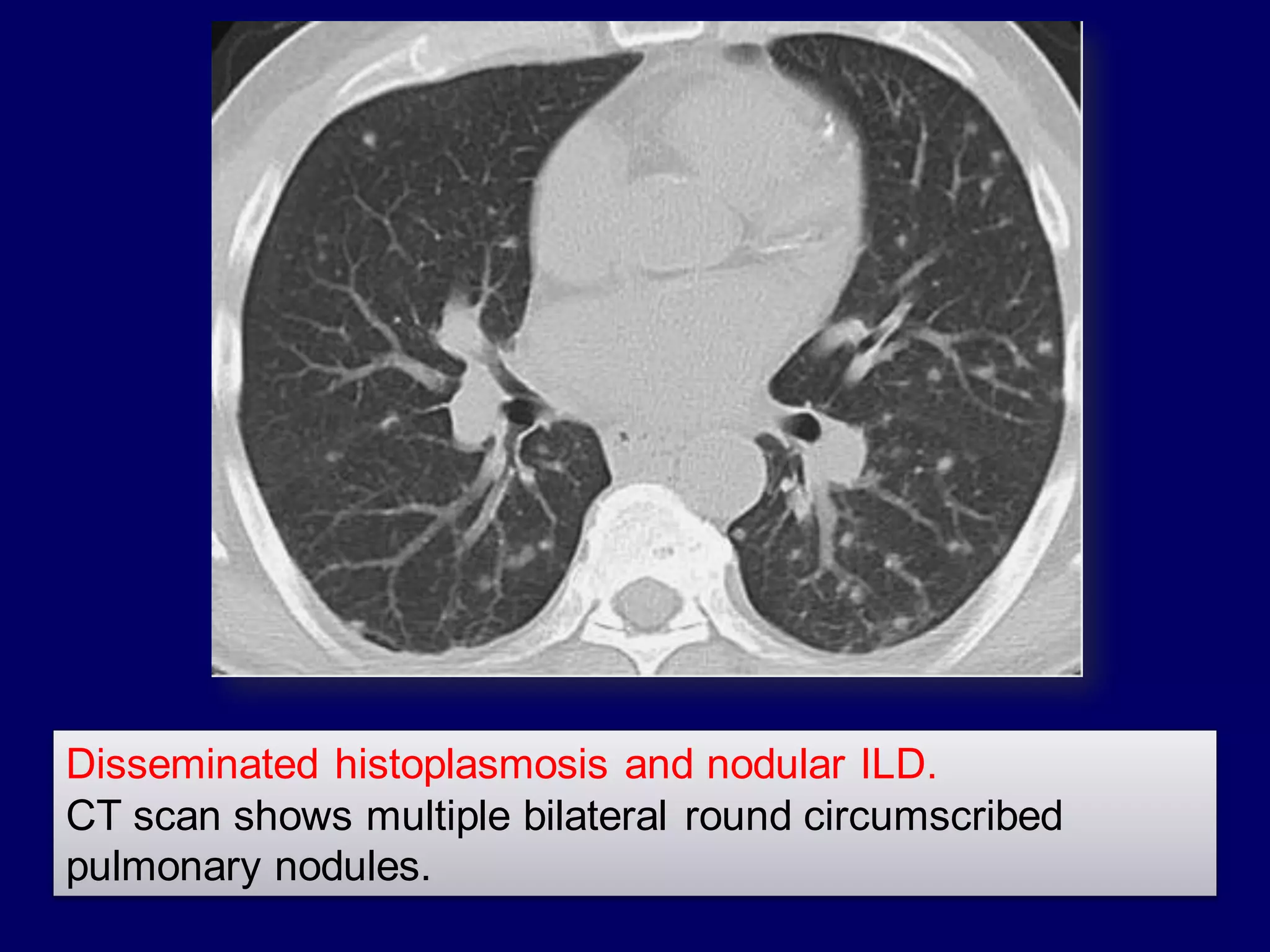
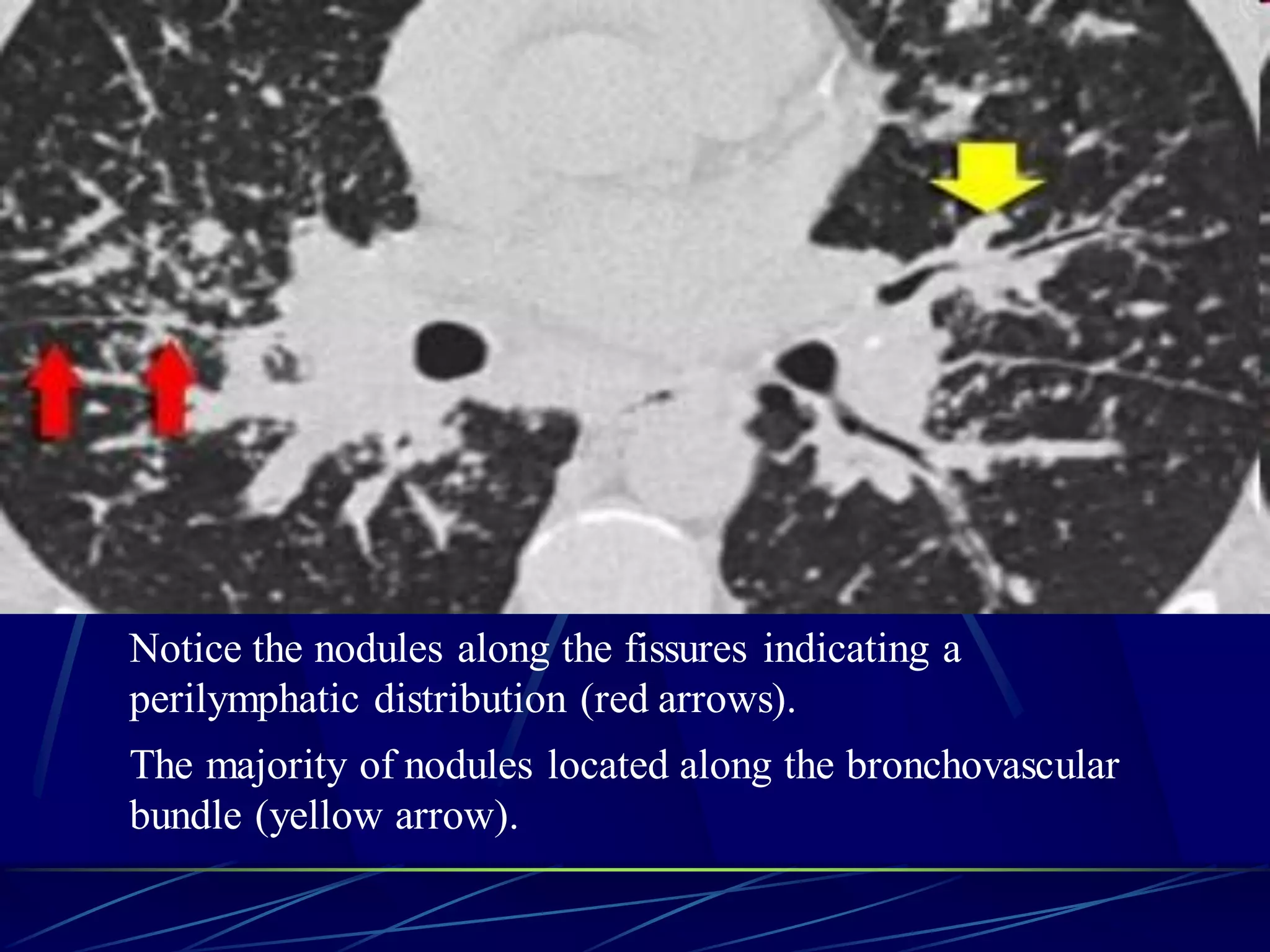
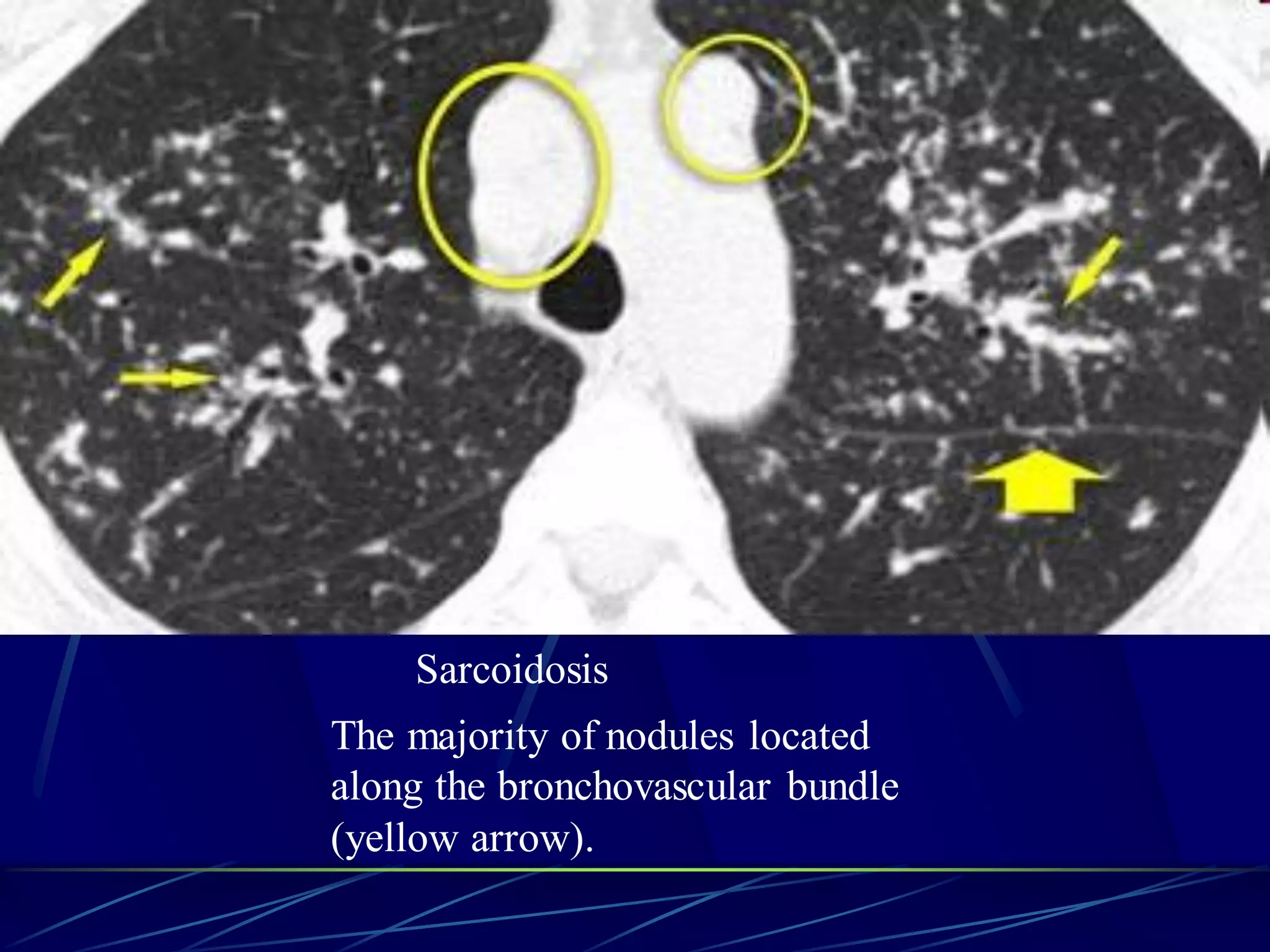
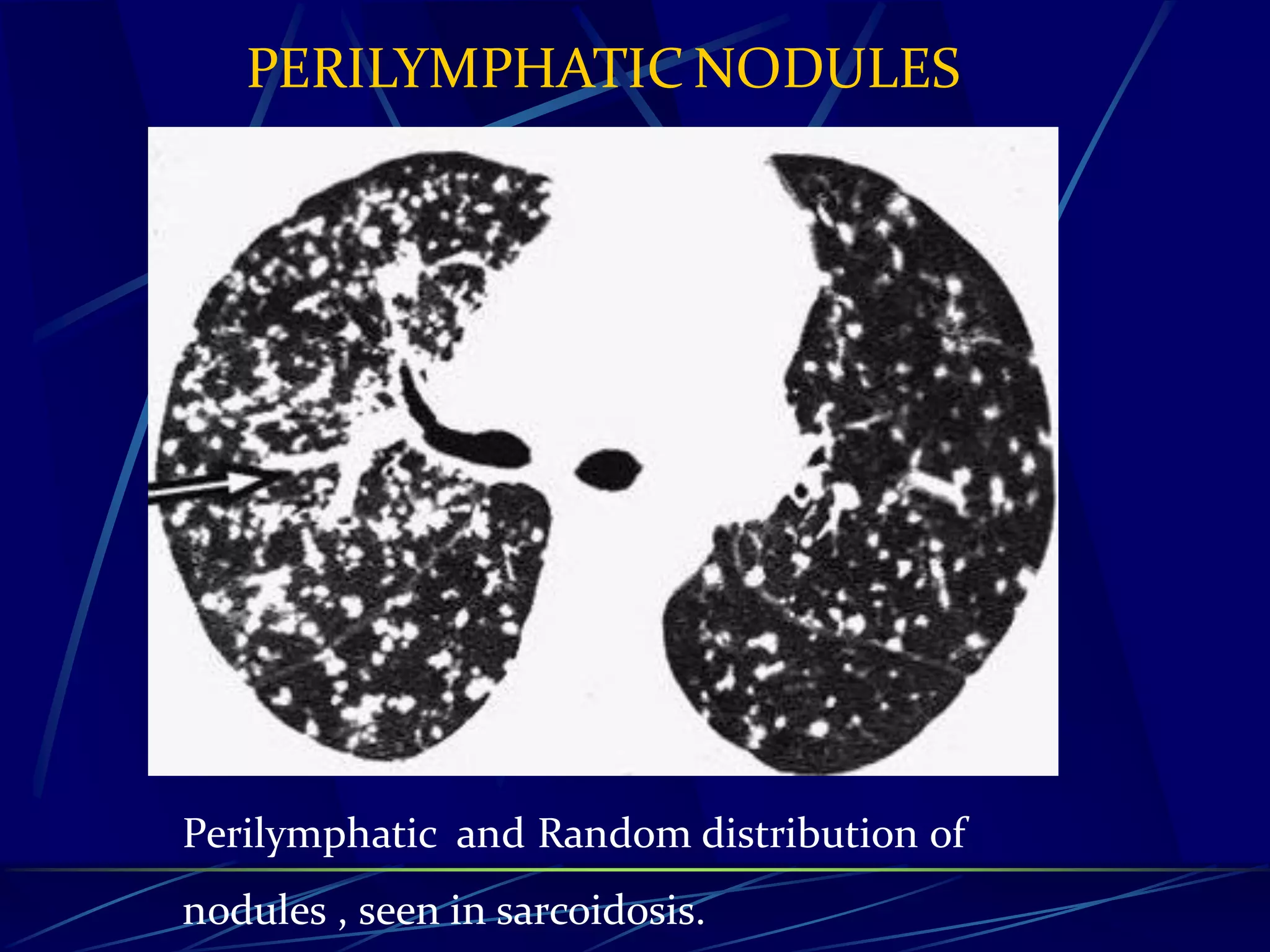
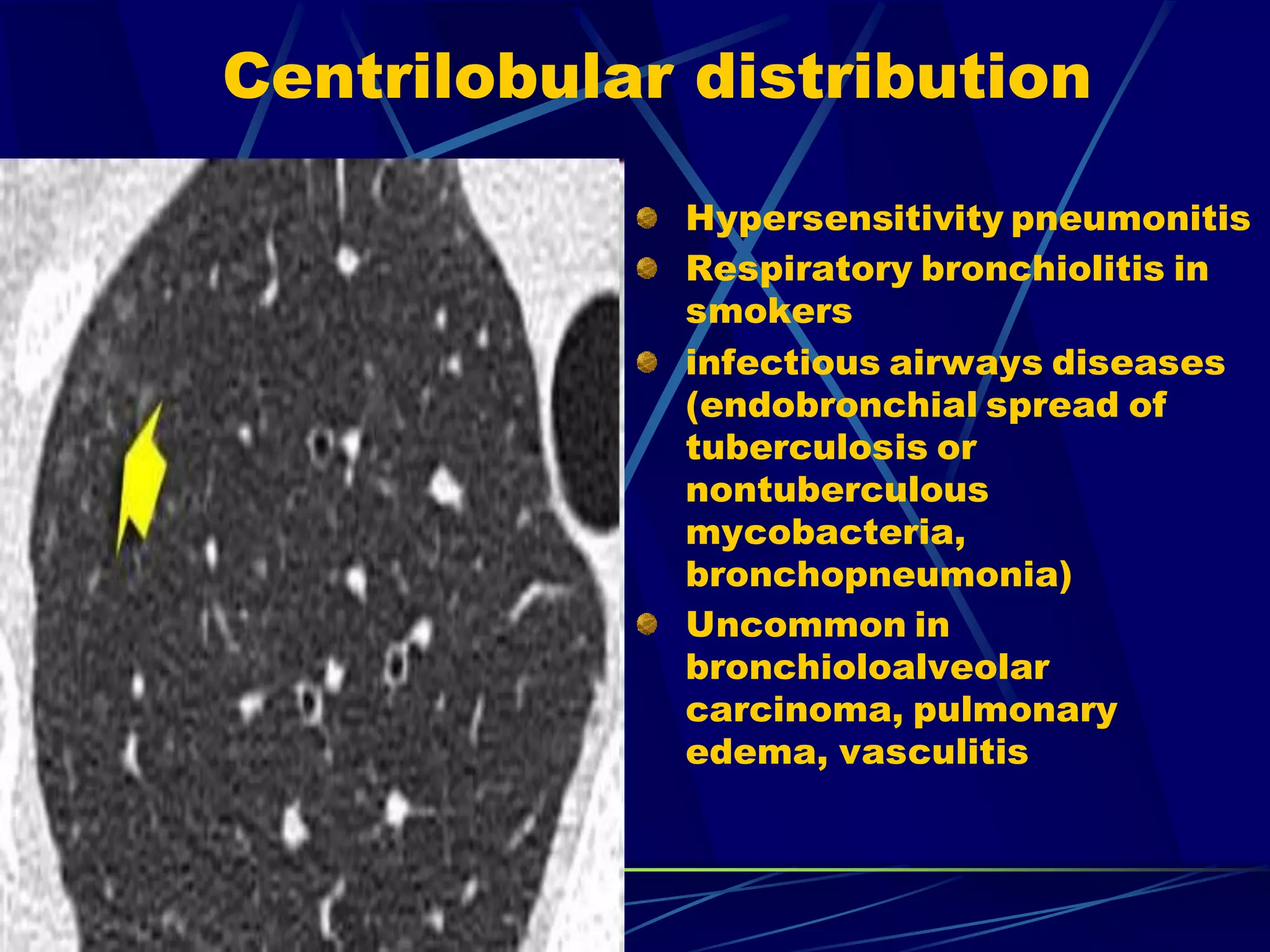
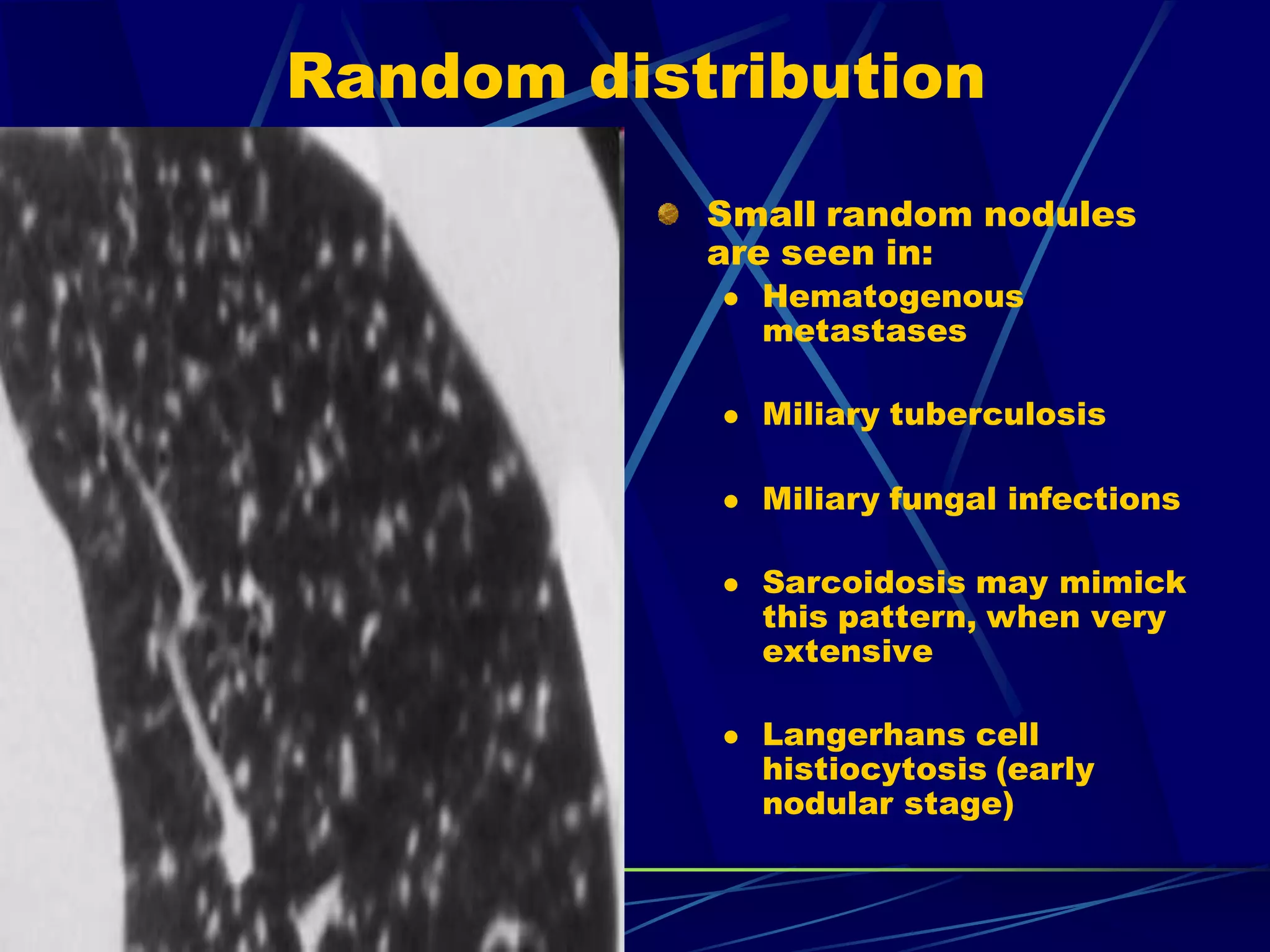
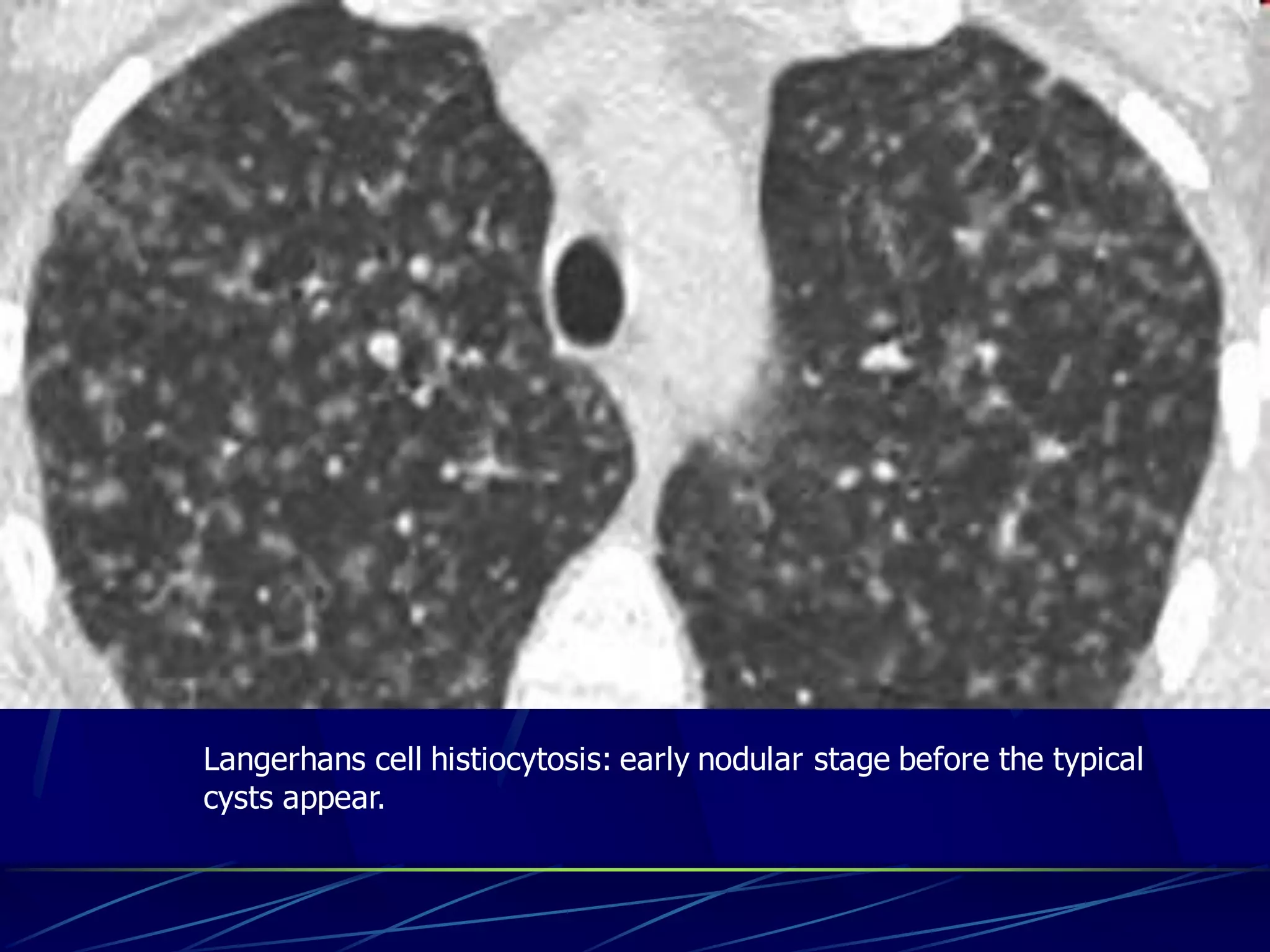


This document discusses nodular patterns seen on chest imaging. It defines nodular opacities as round opacities 1 mm to 1 cm in diameter. Nodular patterns can be described by size, distribution, and appearance. Distribution is classified as perilymphatic along lymphatic vessels and pleura, centrilobular around central lobular structures, or random. Differential diagnoses are suggested based on distribution and other characteristics. A reticulonodular pattern contains both reticular and nodular opacities and requires considering causes of both patterns.























































































