«Δυσλιπιδαιμία», Webinar της ΕΔΕ (5/11/2014) και η εισηγήτρια που θα το παρουσιάσει είναι η κα. Μαρίνα Νούτσου, Διευθύντρια της Β’ Πανεπιστημιακής Π
«Δυσλιπιδαιμία» webinar της ΕΔΕ (5/11/2014) από την κα. Μαρίνα Νούτσου, Διευθύντρια της Β’ Πανεπιστημιακής Παθολογικής Κλινικής του Διαβητολογικού Κέντρου ΓΝΑ “Ιπποκράτειο”
Similar to «Δυσλιπιδαιμία», Webinar της ΕΔΕ (5/11/2014) και η εισηγήτρια που θα το παρουσιάσει είναι η κα. Μαρίνα Νούτσου, Διευθύντρια της Β’ Πανεπιστημιακής Π
Οδηγίες για τηνφαρμακευτική αντιμετώπιση
της δυσλιπιδαιμίας
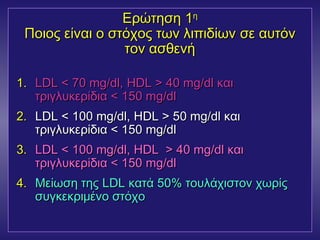
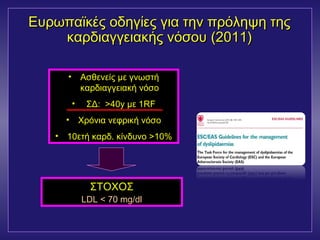
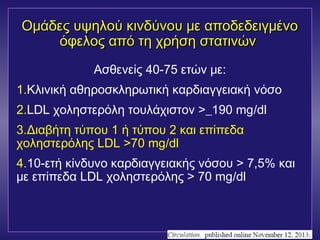
1ος στόχος θεραπείας: LDL
1η επιλογή: Στατίνες
AHA 2001
American Diabetes Association. Position Statement. Diabetes Care 2014; 37(Suppl 1): S14-S80
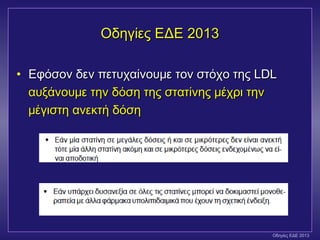
Ελληνική Διαβητολογική Εταιρεία 2013
#3 Slide 13. Dyslipidemia in Diabetes
As described in the preceding slides, high triglyceride and high VLDL levels lead to low HDL, fewer HDL particles, and small, dense LDL.
#26 Potential time course of statin effects
CHD risk reduction with a statin appears to occur as a result of several related changes, including restoration of endothelial function, reduction in inflammation, and stabilization of vulnerable plaque. The time course for these antiatherosclerotic effects of statins ranges from days to years. Within weeks to months after beginning statin therapy, endothelial function of coronary arteries is restored. Concurrent with this or following by just a few months is a reduction in inflammatory markers, such as high-sensitivity C-reactive protein. These effects appear to coincide with the reduction in ischemic events demonstrated after about 18 months of statin therapy. After several years of therapy (i.e., 1.5–2.5 years), fatal and nonfatal myocardial infarction rates begin to decline in statin-treated patients, and after 5 years of therapy, significant reductions have been documented. These changes coincide somewhat with stabilization of vulnerable atherosclerotic plaque during which the lipid-rich core of plaque is replaced with connective tissue and matrix.
#46 Statin plus fibrate combination therapy
Combining a fibrate with a statin raises safety concerns because of the potential for myopathy and overt rhabdomyolysis. However, almost all reports of such adverse effects have been in particular situations, in which one should avoid administering this drug combination. Higher doses of statins, particularly simvastatin 80 mg/d or atorvastatin 80 mg/d, should not be combined with any fibrate. Also, because fibrates are renally excreted, plasma levels are increased in patients with renal insufficiency, thereby increasing the risk for drug–drug interactions. In addition, the combination of a fibrate and a statin should not be used with agents that interfere with clearance of statins because the statin will then interact with the fibrate; the immunosuppressive agent tacrolimus may also have this effect. Finally, because of problems with renal and hepatic function, patients older than 70 years should not be treated with a fibrate plus a statin.