

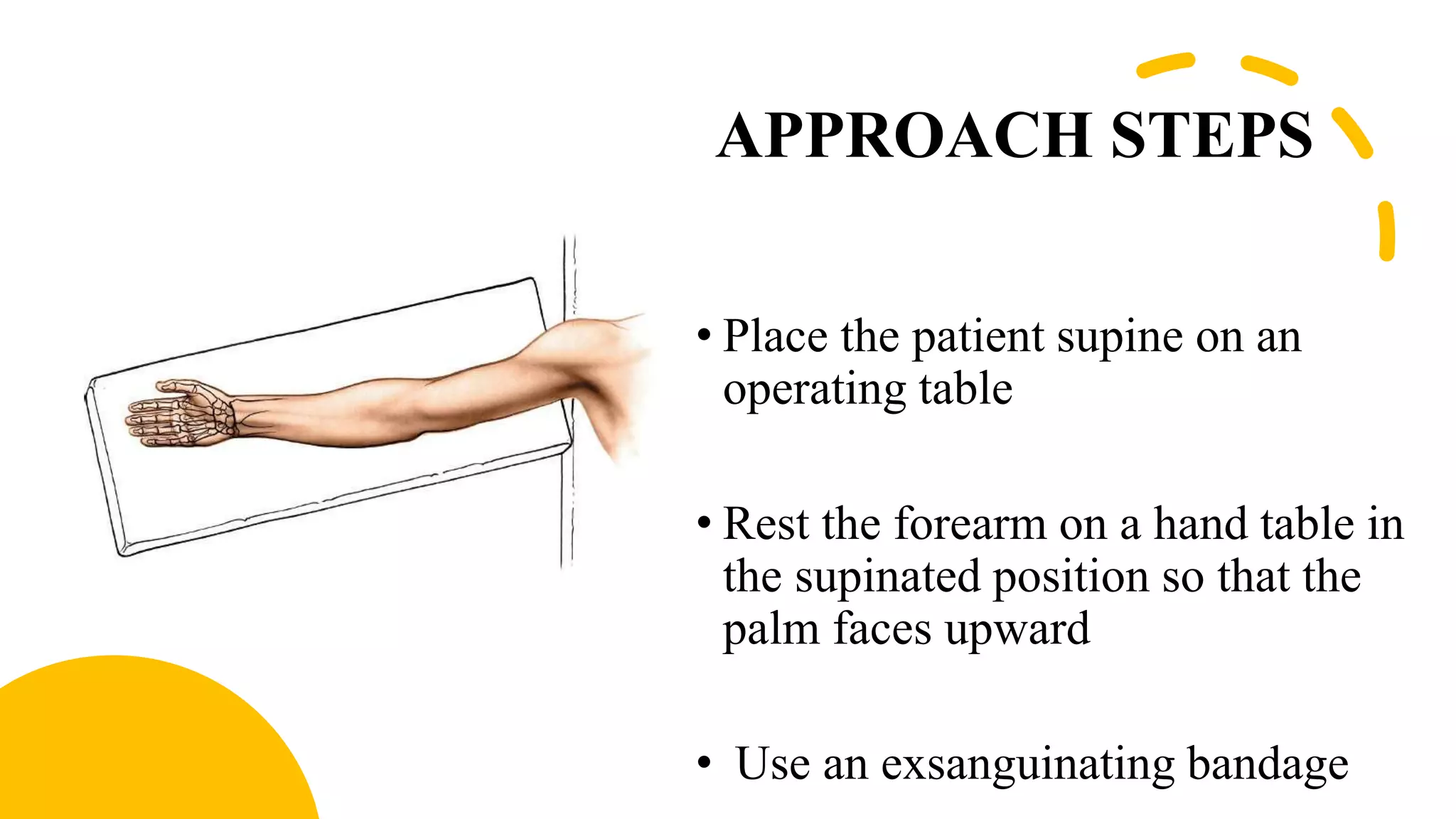

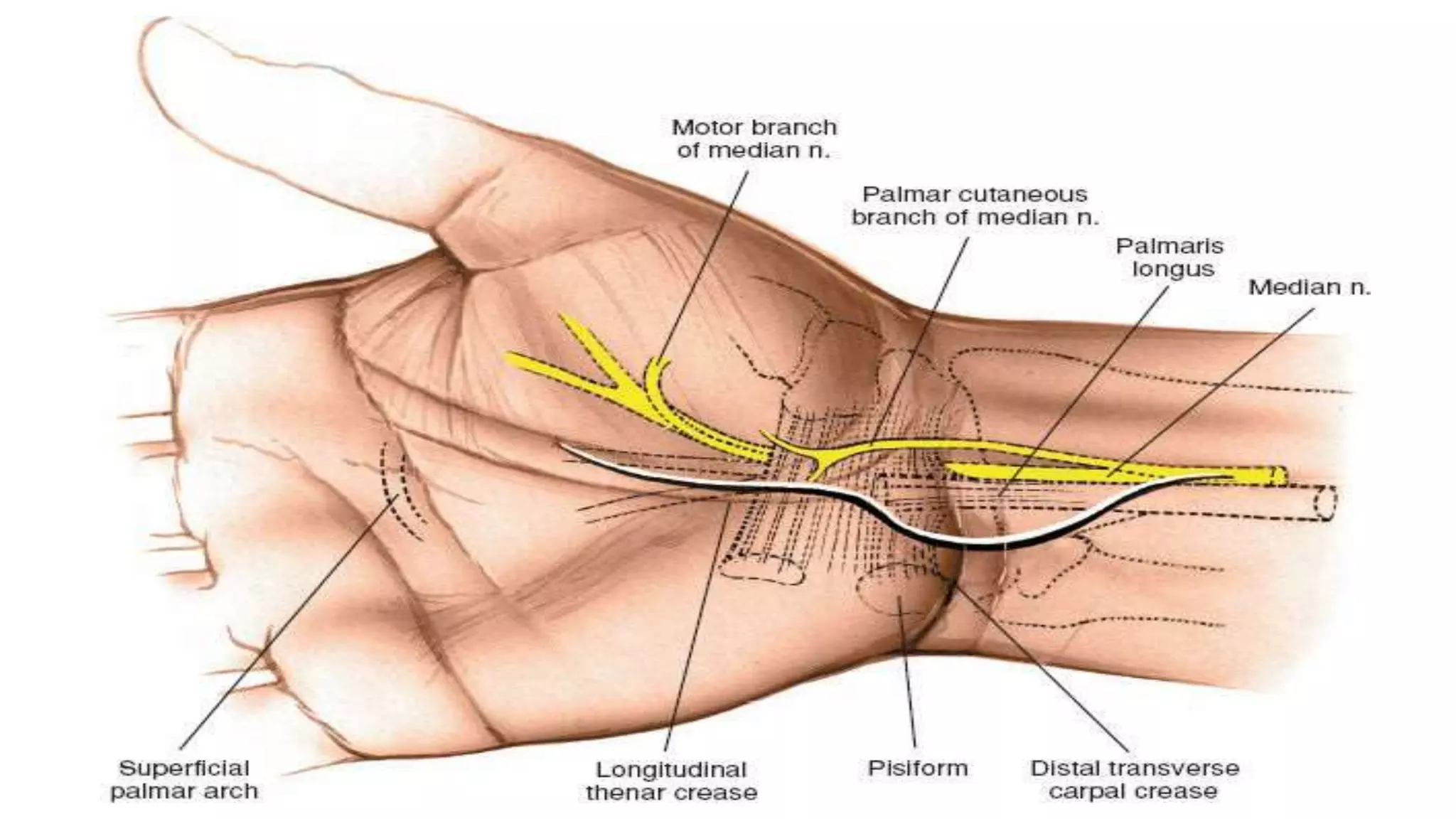
















This document provides an overview of the volar approach to the wrist. It begins with an introduction and objectives. The indications for the volar approach include carpal tunnel release, tendon repair, and fixation of distal radius fractures. The approach steps are then described, including making a curved incision just ulnar to the thenar crease. Key structures at risk include the palmar cutaneous branch of the median nerve and the motor branch to the thenar muscles. Other volar approaches and an accompanying video are also mentioned.












































































