Downloaded 19 times



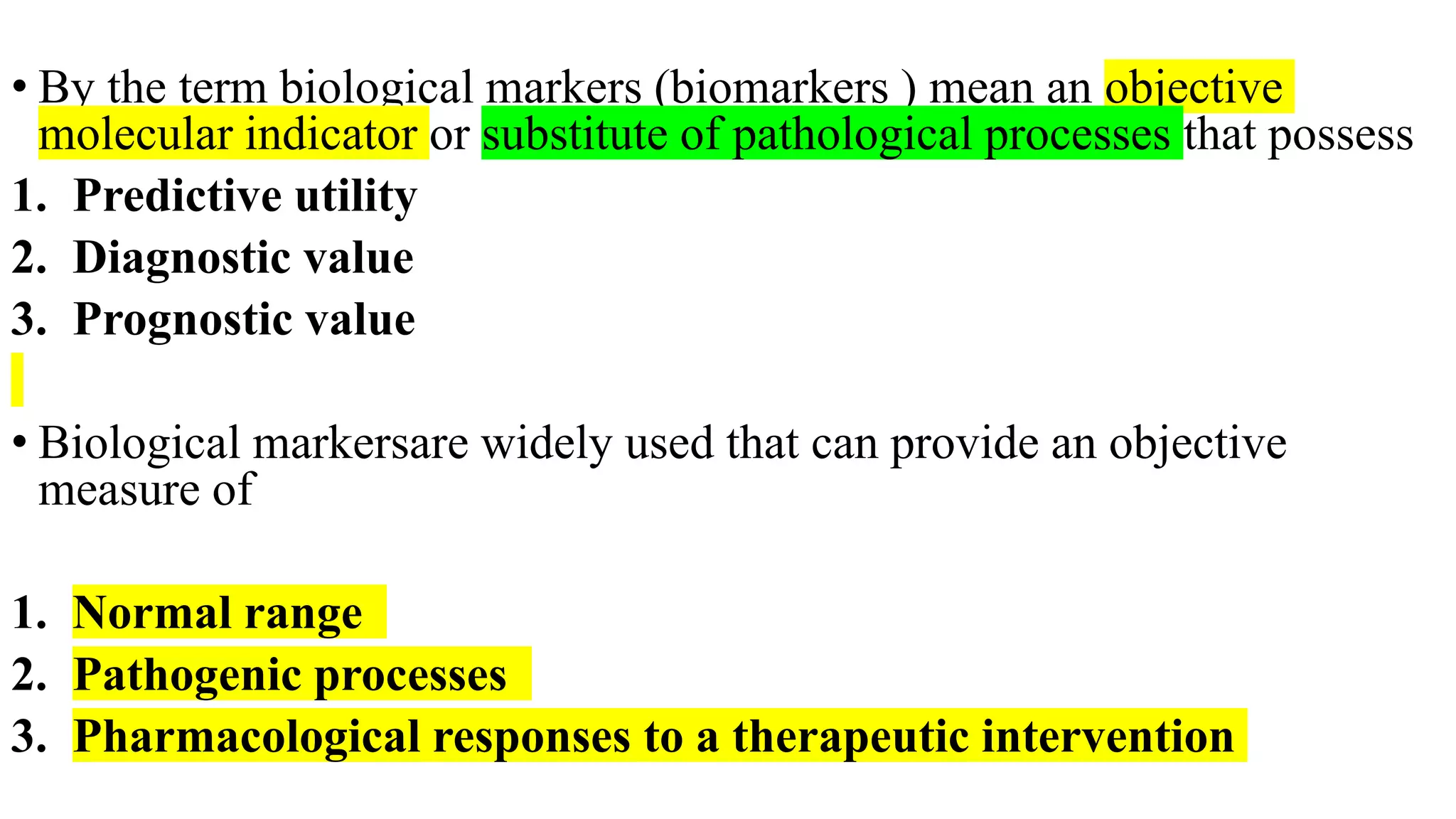








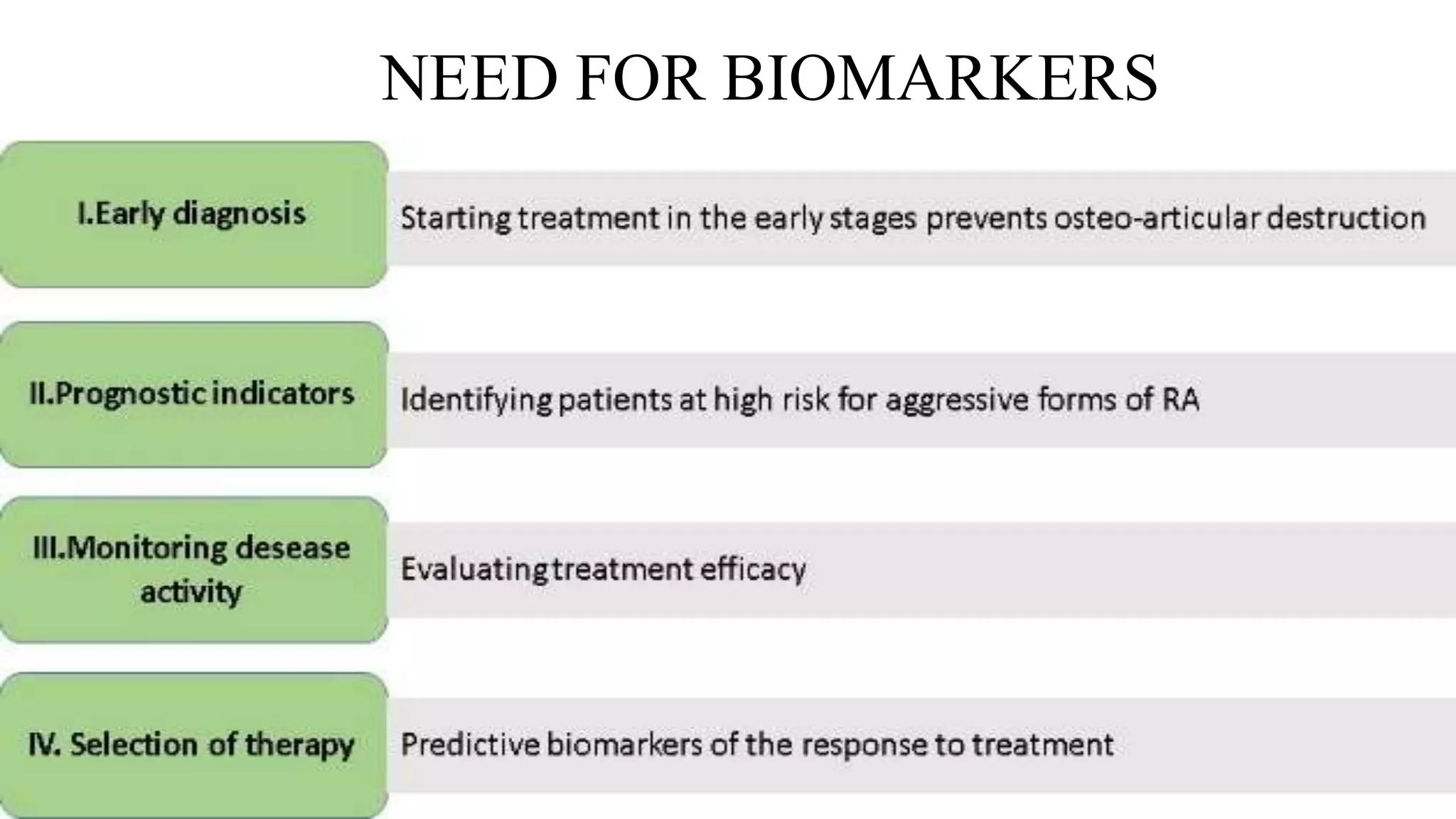





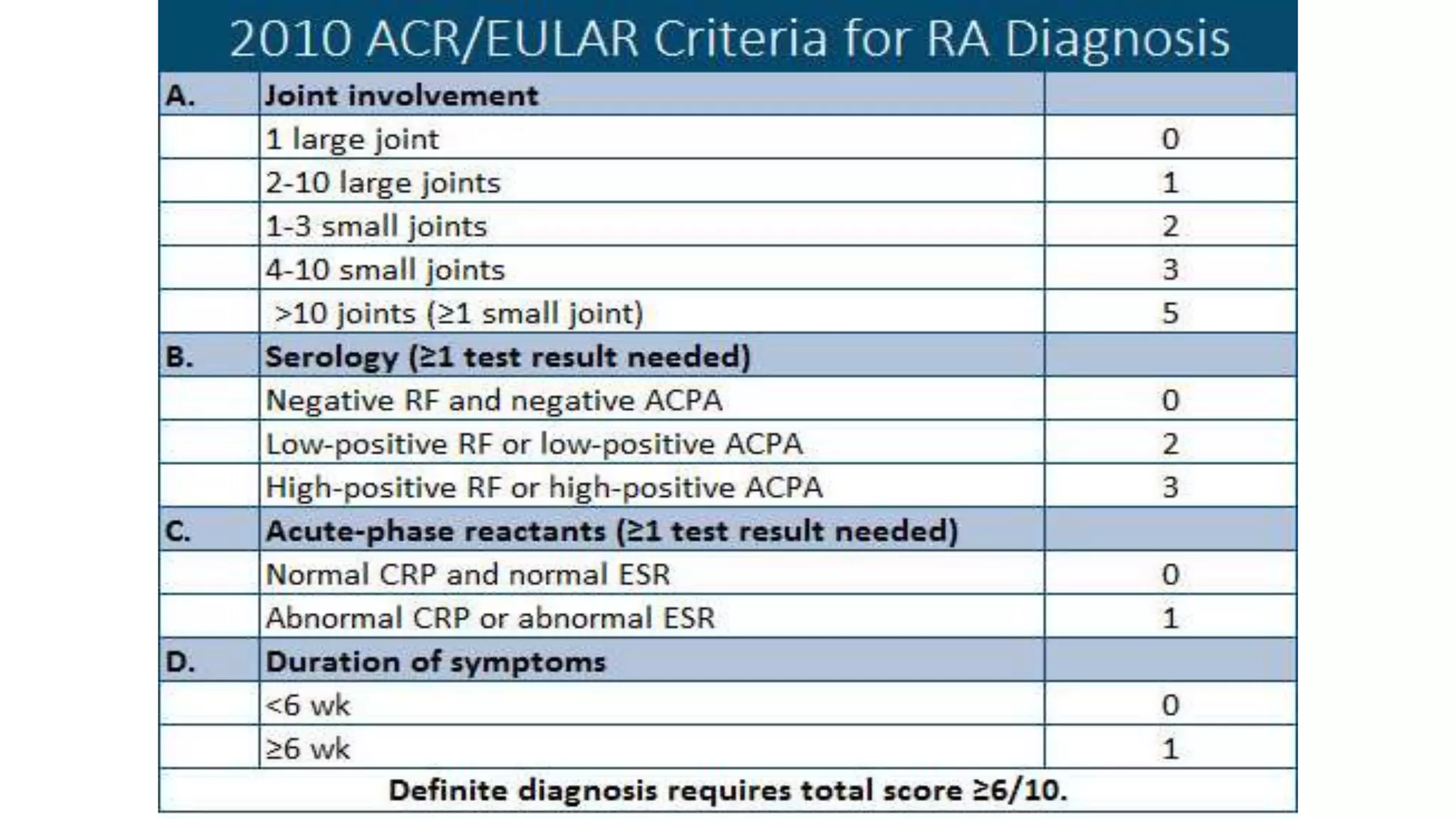





































This document presents an extensive overview of biological markers in rheumatology, focusing on their diagnostic, prognostic, and monitoring roles specifically in rheumatoid arthritis (RA). It details various biomarkers, including rheumatoid factor, anti-CCP, and newer markers like 14-3-3 eta protein and anti-MCV antibodies, as well as the use of multi-biomarker disease activity tests to assess disease activity and predict responses to biologic therapies. The lesson aims to educate students on the importance of these biomarkers in the identification and management of RA.












































































