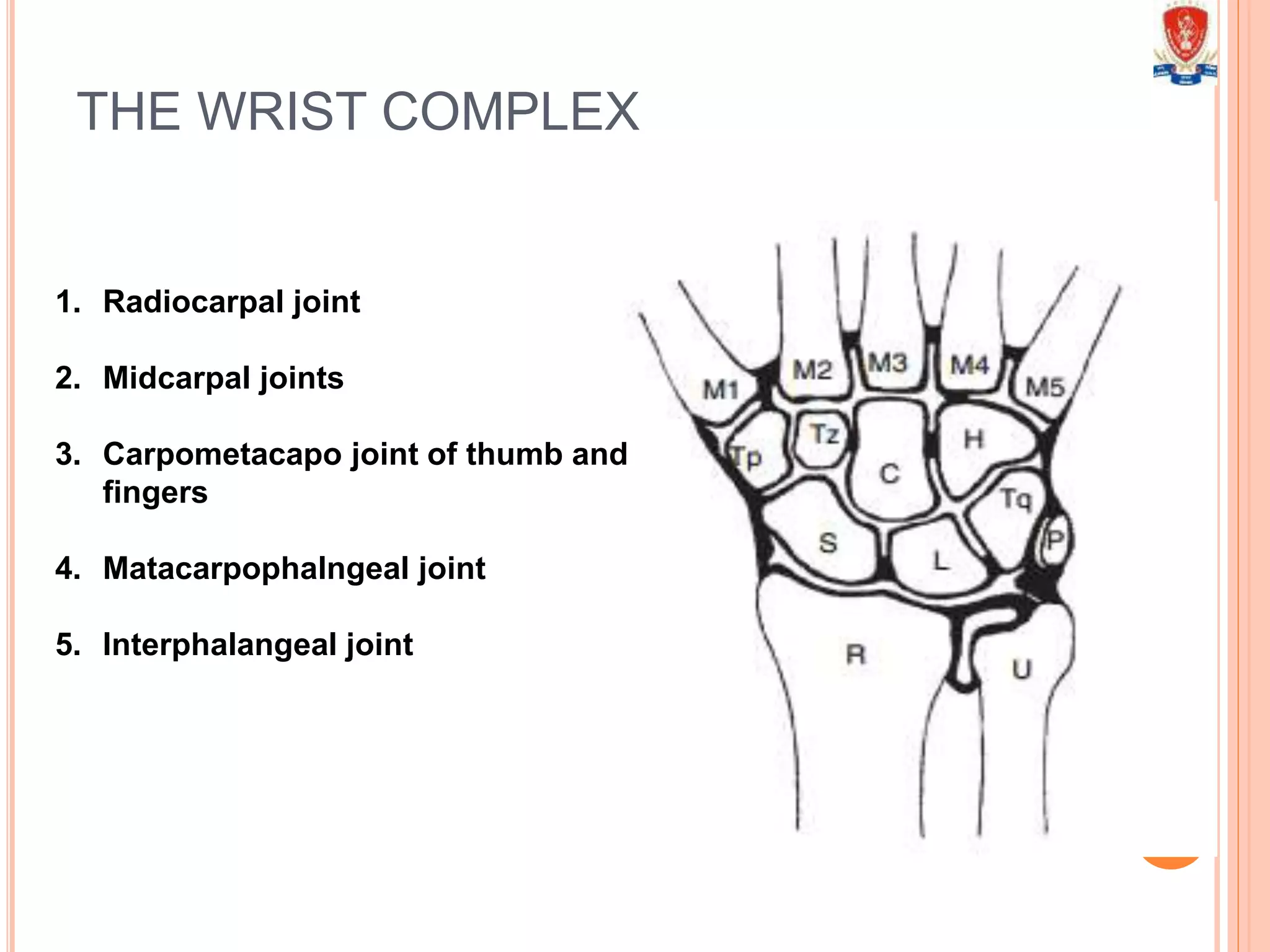
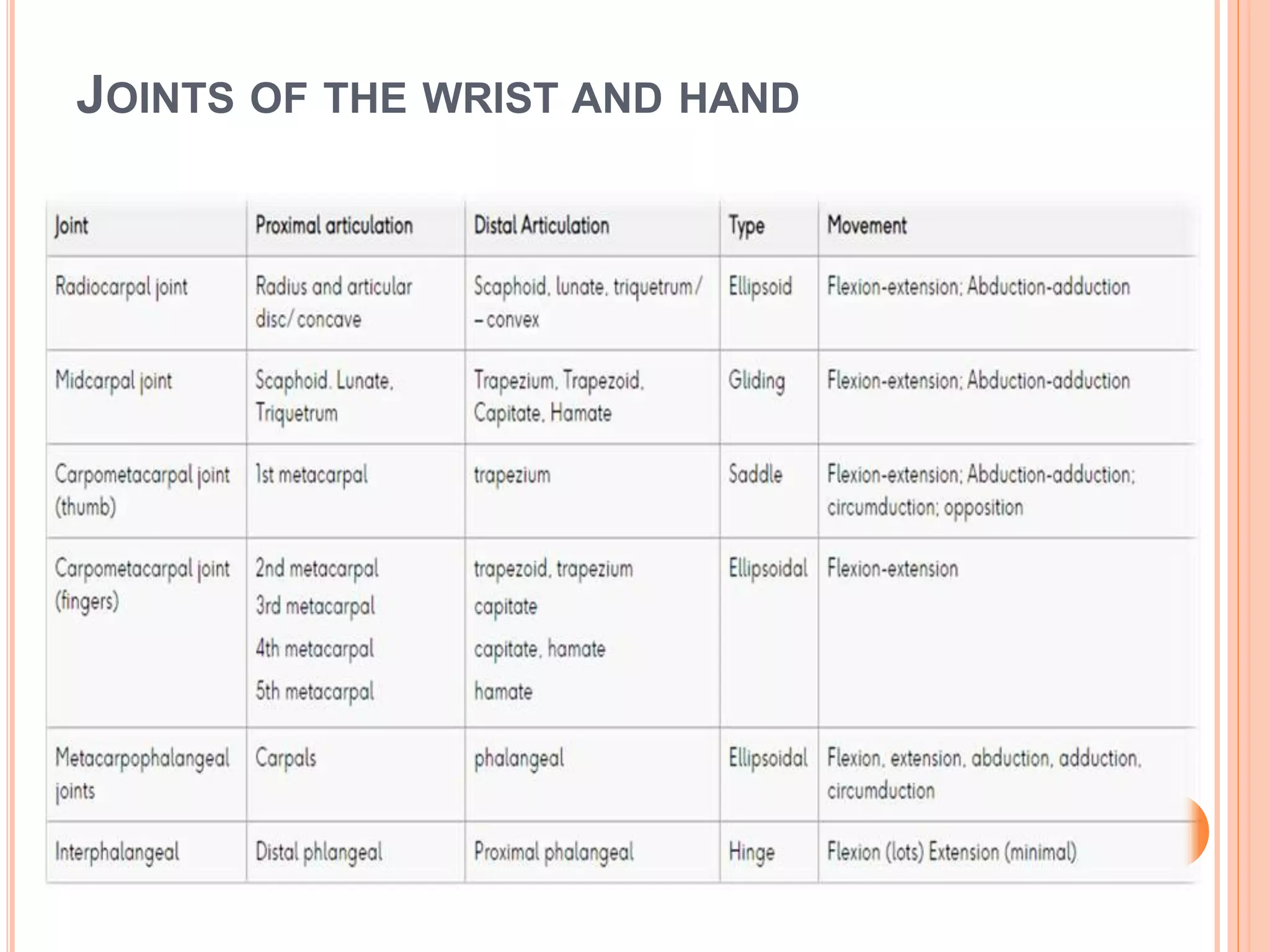
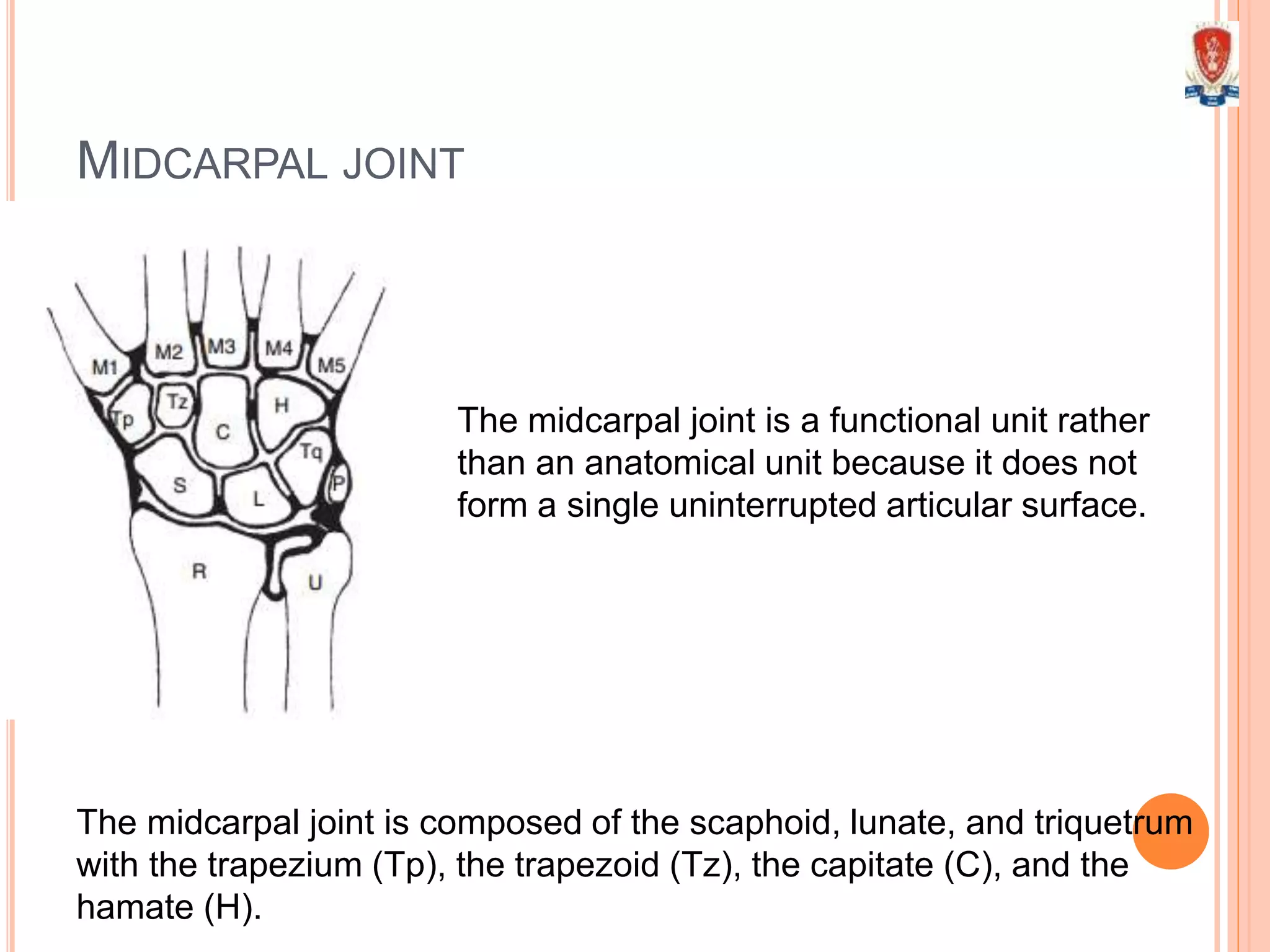
1) The wrist joint complex includes the radiocarpal joint between the radius and proximal carpal row, midcarpal joints between the proximal and distal carpal rows, and carpometacarpal joints of the thumb and fingers.
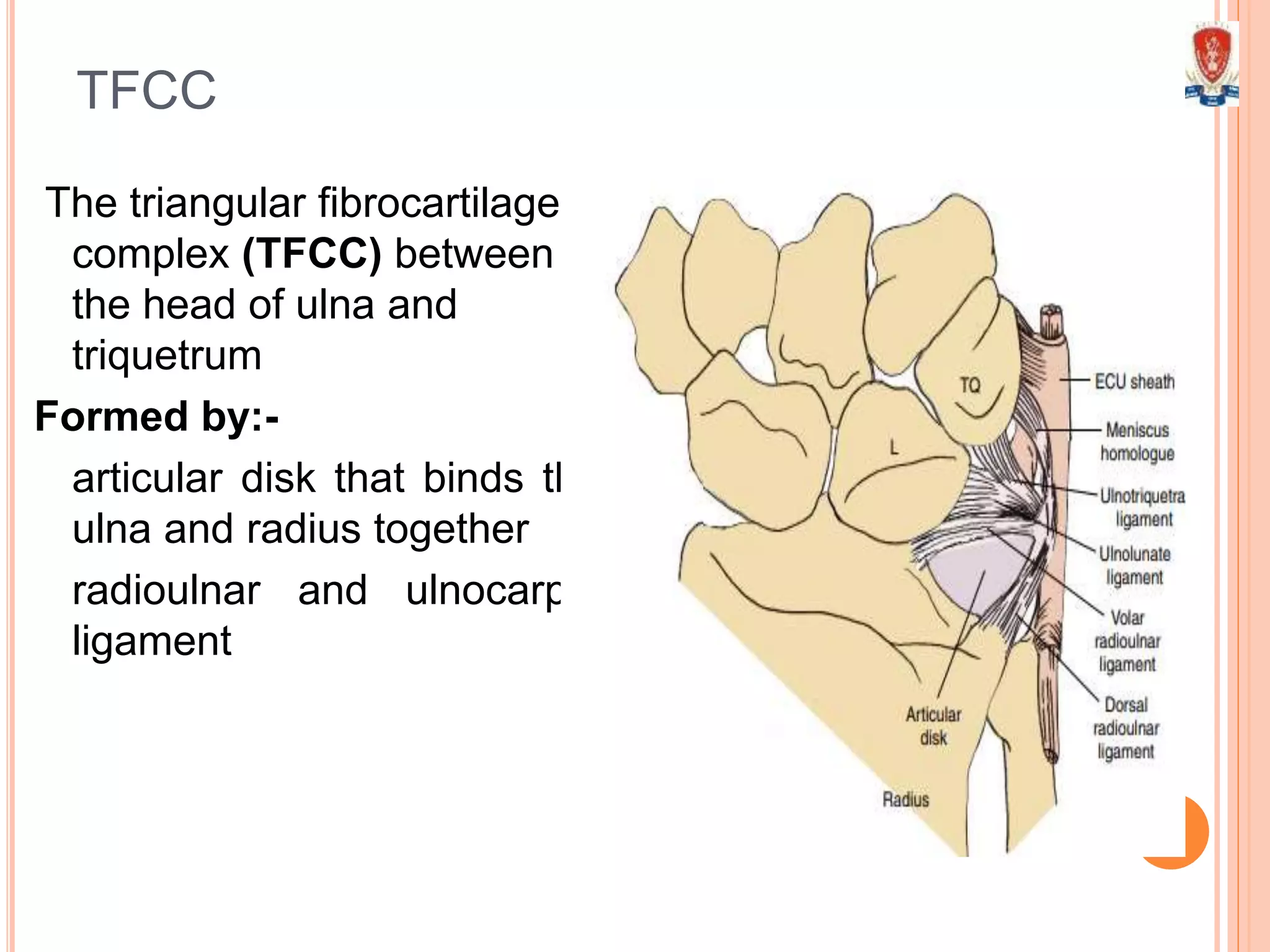
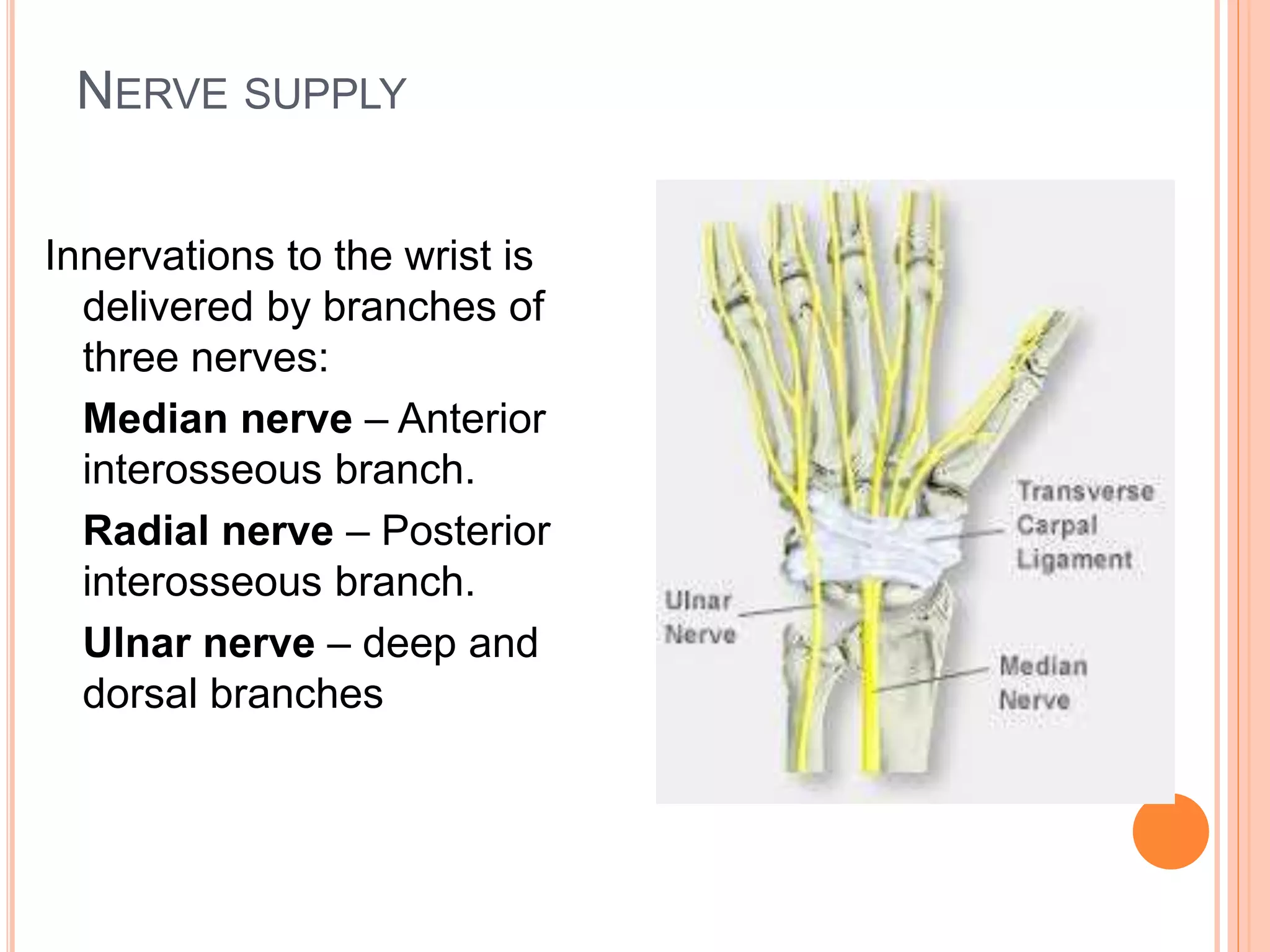
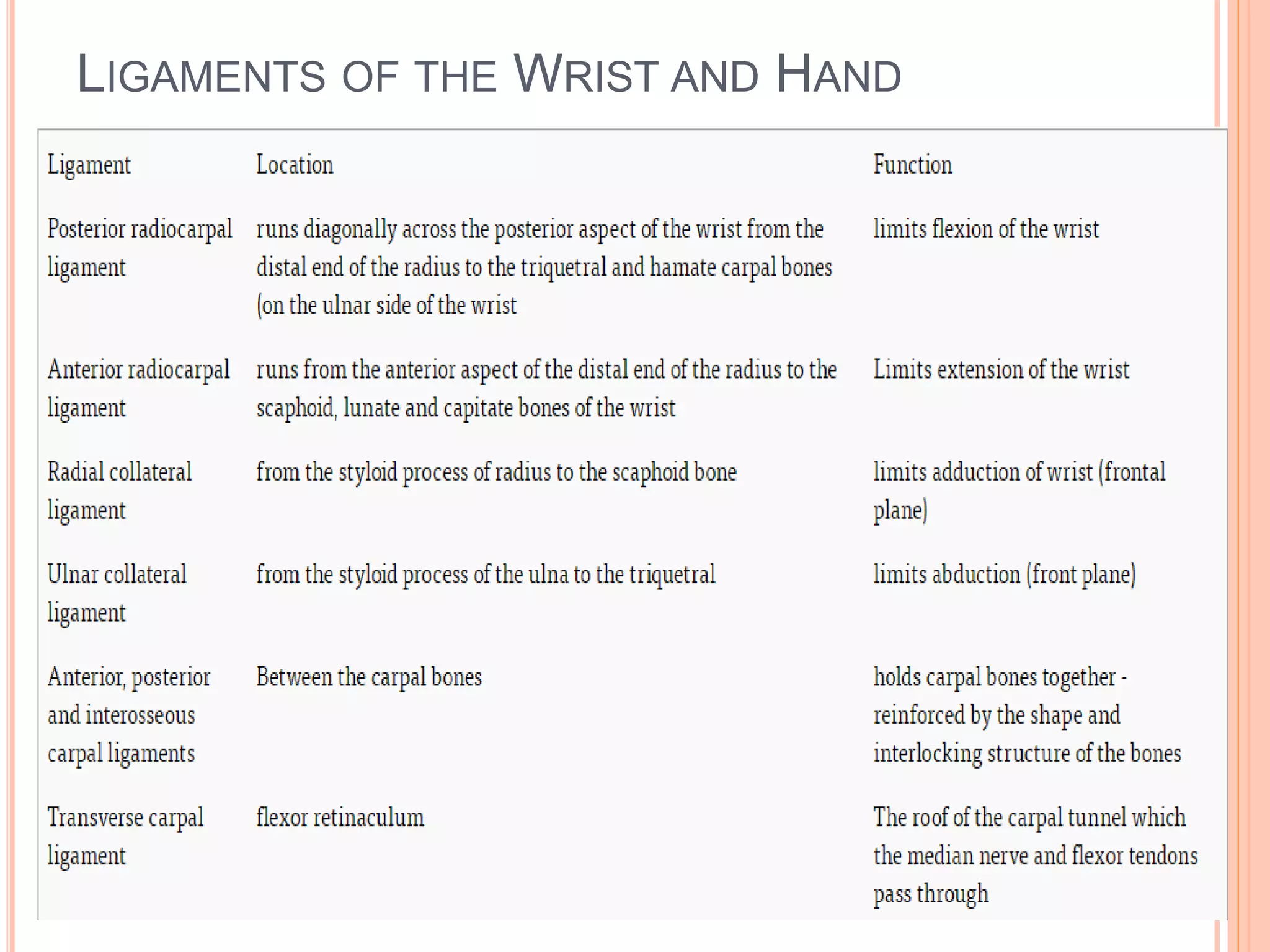
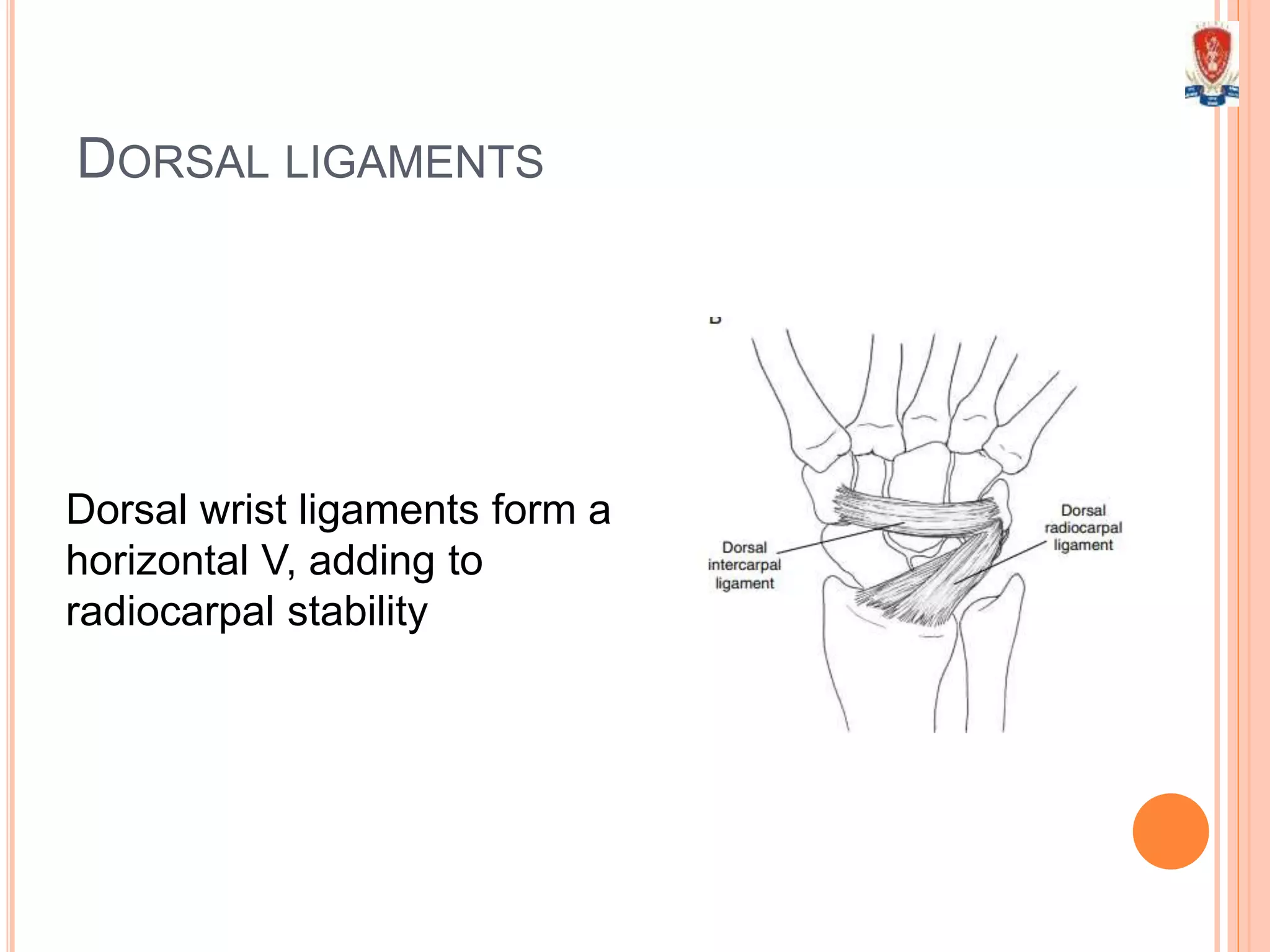
2) Key structures include the triangular fibrocartilage complex between the ulna and triquetrum bone, ligaments such as the radiocarpal and intercarpal ligaments, joint capsules, and muscles that cross the wrist including flexors and extensors.
3) The document describes the bones, joints, ligaments, muscles, movements, blood supply and common injuries of the wrist complex in detail.