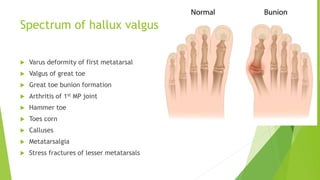
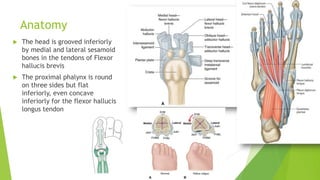
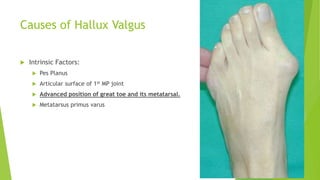
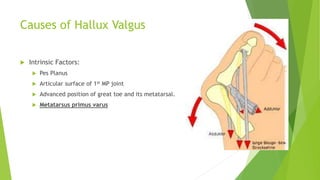
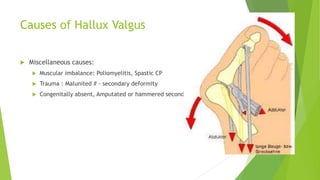
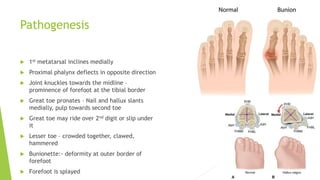
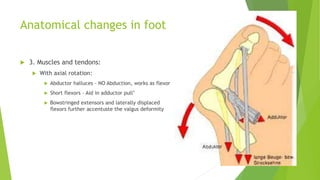
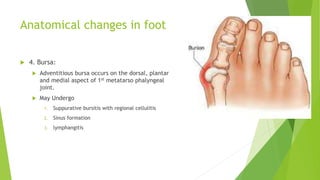
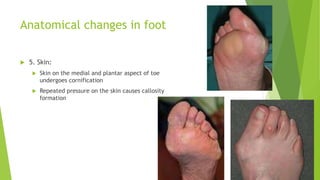
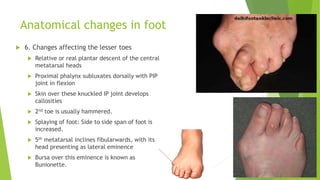
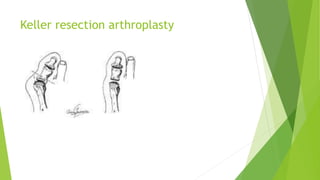
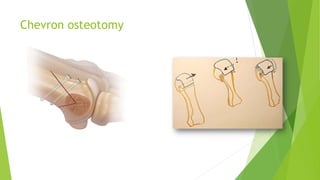
Hallux valgus, or a deviated great toe, is a common foot deformity. It involves the lateral deviation of the great toe with valgus of the first metatarsal. It can cause pain and make shoe wearing difficult. While small deformities may be treated with proper shoes, surgery is often needed for more severe cases to realign bones and tissues. The document discusses the anatomy, causes, classifications, symptoms, investigations and various surgical procedures used to treat hallux valgus.