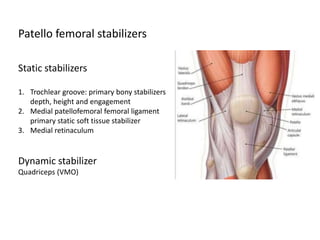
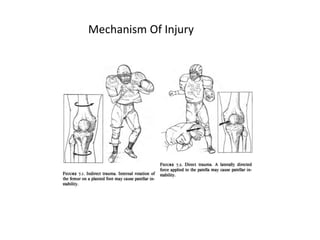
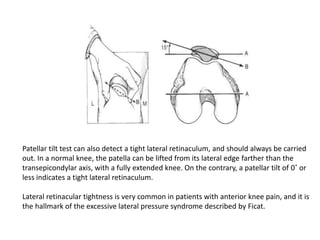
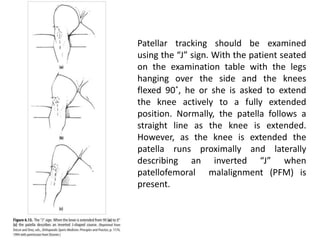
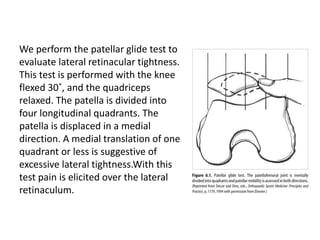
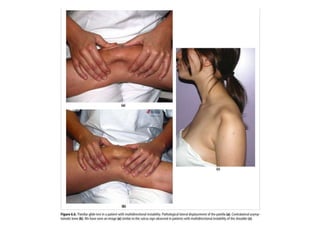
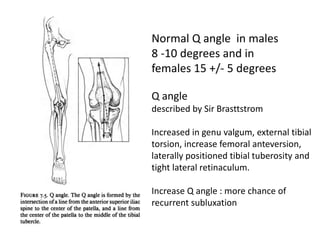
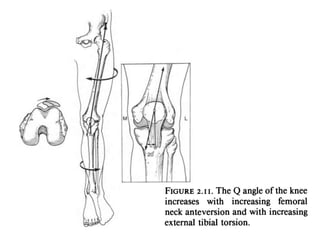
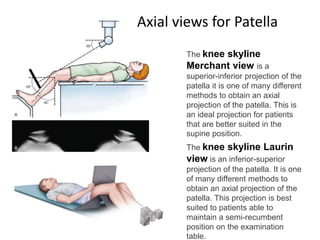
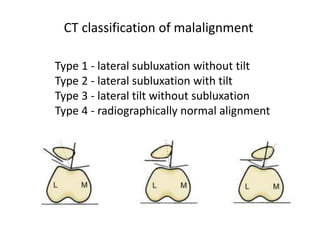
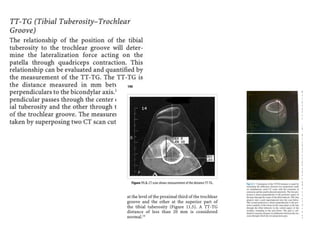
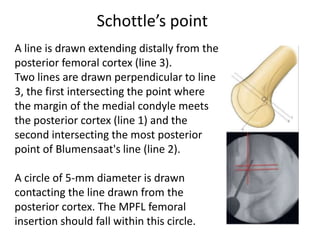
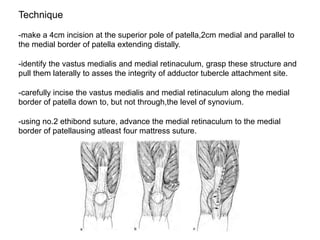
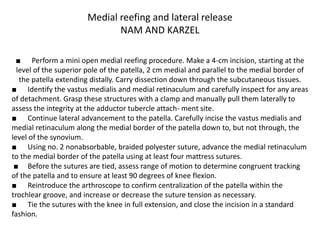
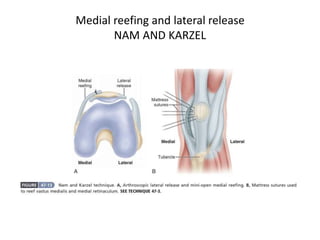
The document discusses patellar dislocations, focusing on anatomy, types of dislocation, evaluation, imaging, and management strategies for patellar instability. It highlights the importance of the medial patellofemoral ligament (MPFL) as a primary stabilizer and details both non-operative and surgical interventions for managing acute and recurrent dislocations. The document emphasizes the role of anatomical variations, such as patella alta and trochlear dysplasia, in predispositions to instability and outlines both diagnostic tests and treatment protocols.