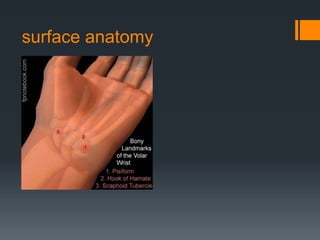
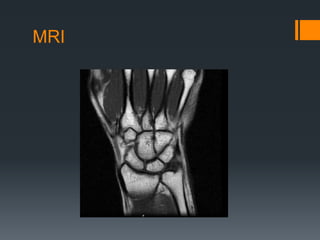
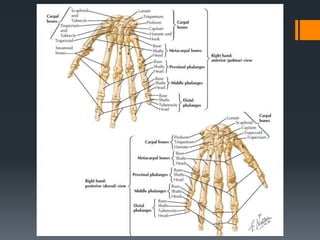
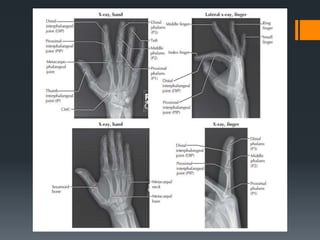
The document provides a comprehensive overview of the anatomy, biomechanics, and clinical examination techniques related to the hand and wrist. It covers detailed aspects such as joint articulations, ligaments, tendons, muscle functions, and neurological and vascular supply, emphasizing important conditions like carpal tunnel syndrome. It also includes assessment methods and relevant diagnostic tests for evaluating hand and wrist injuries.