Download to read offline



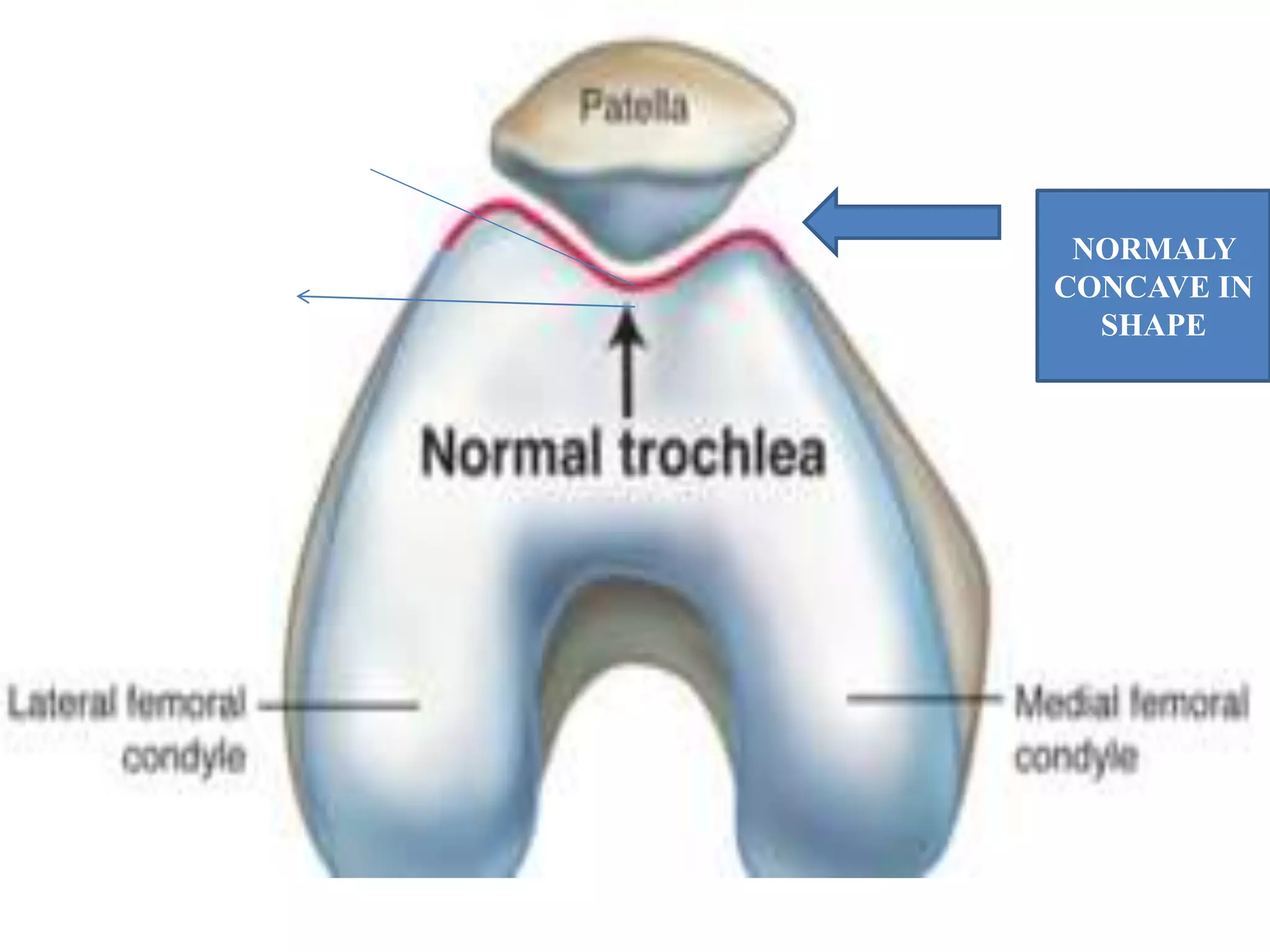

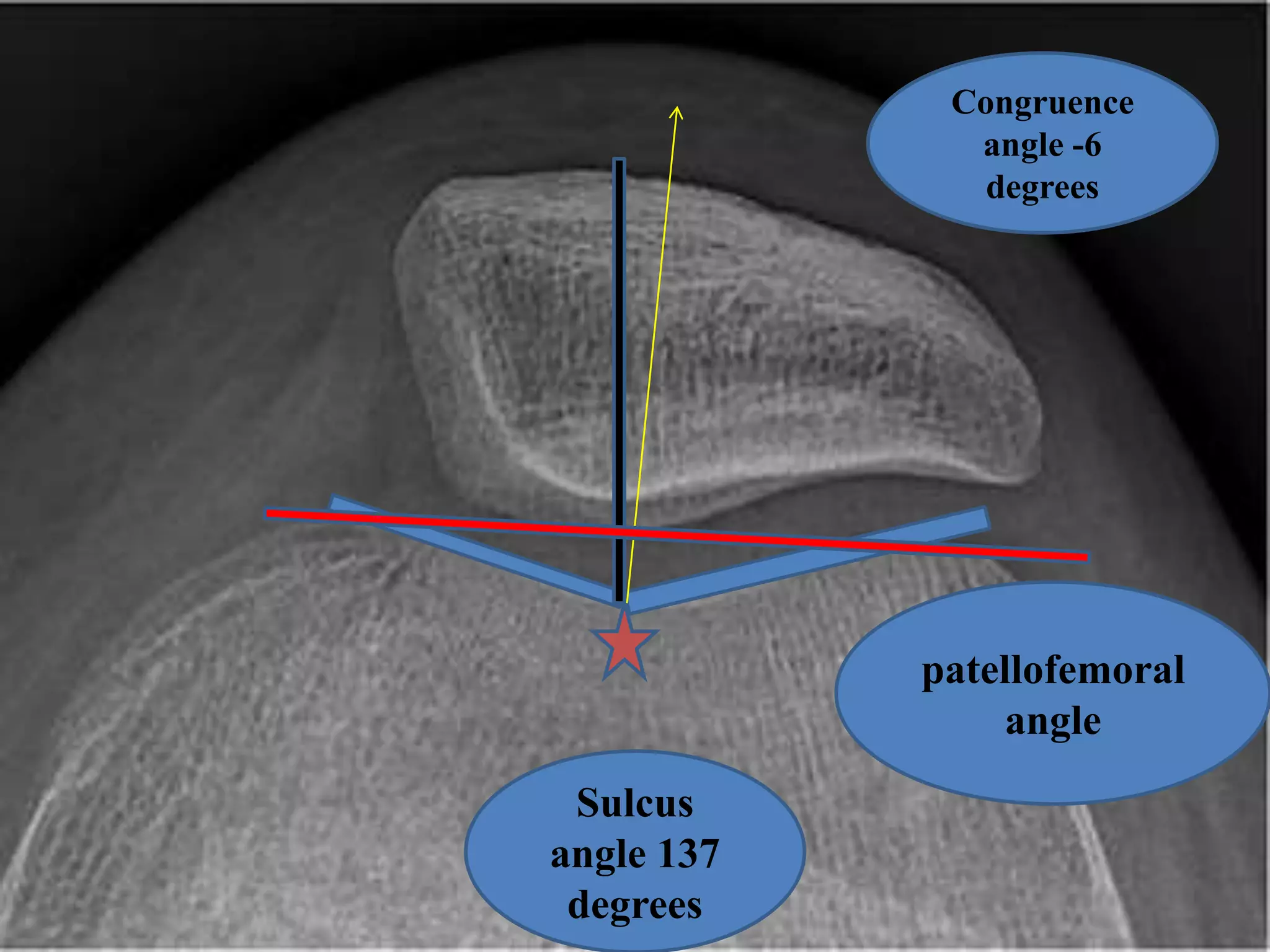

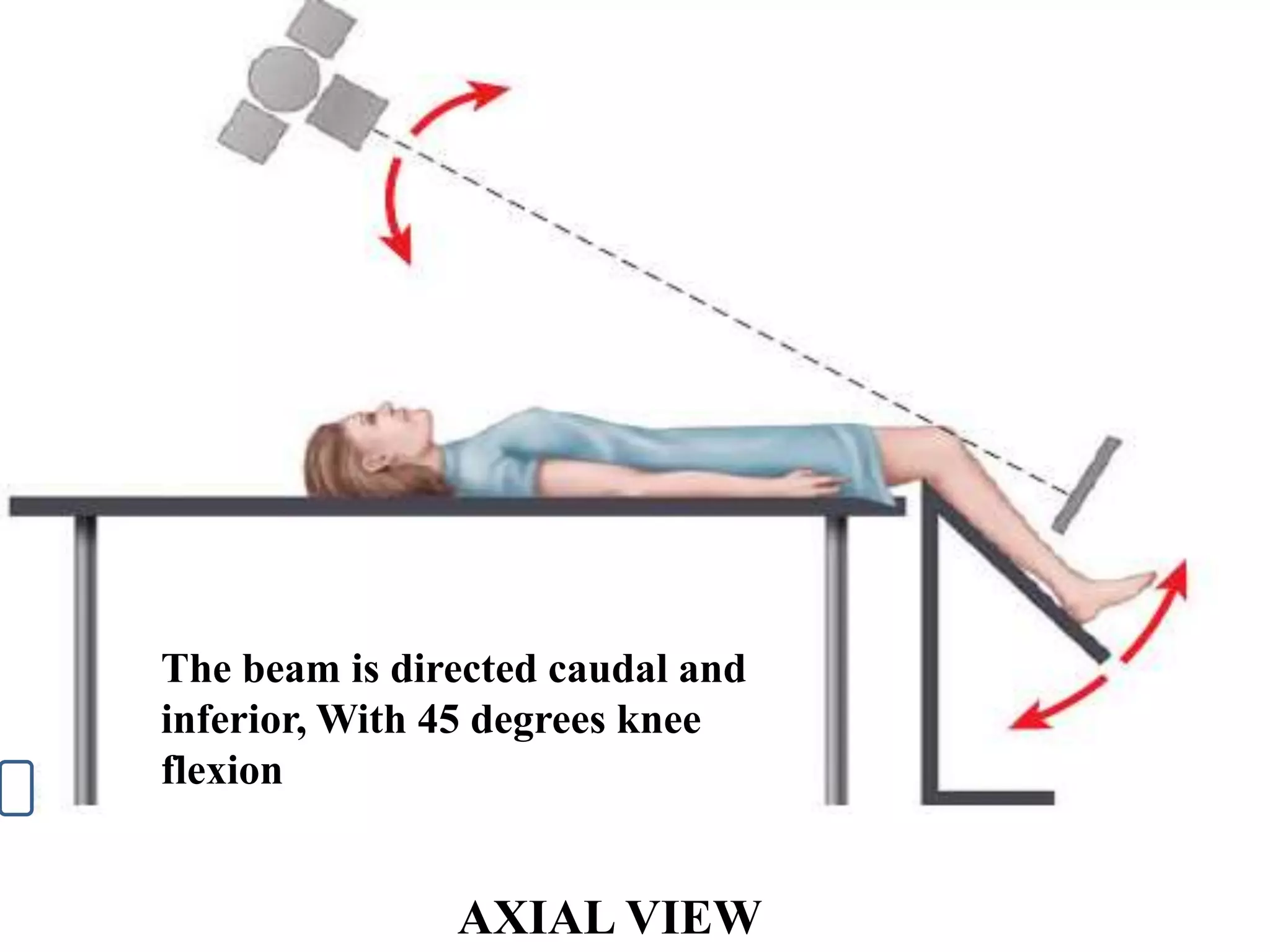


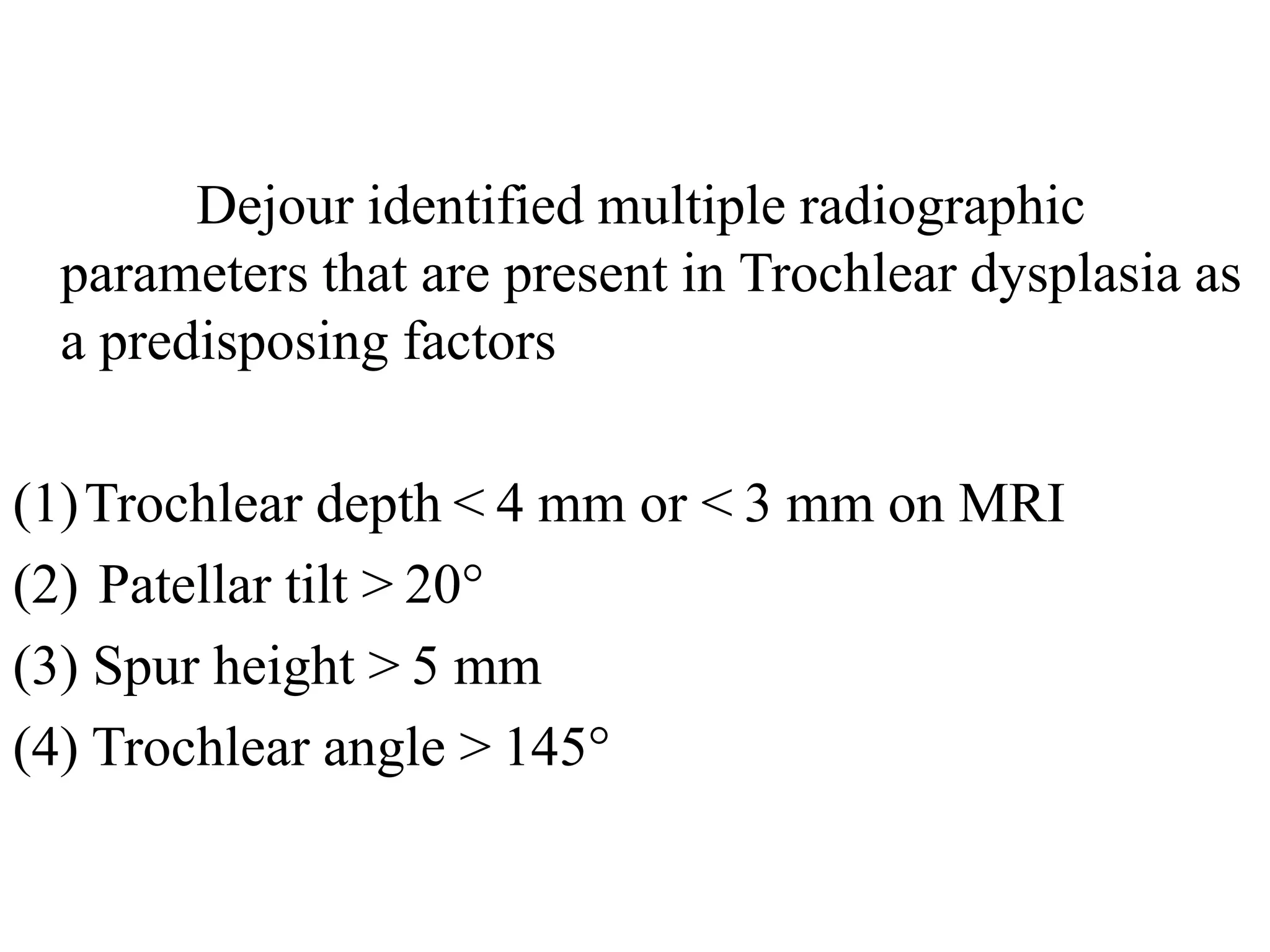


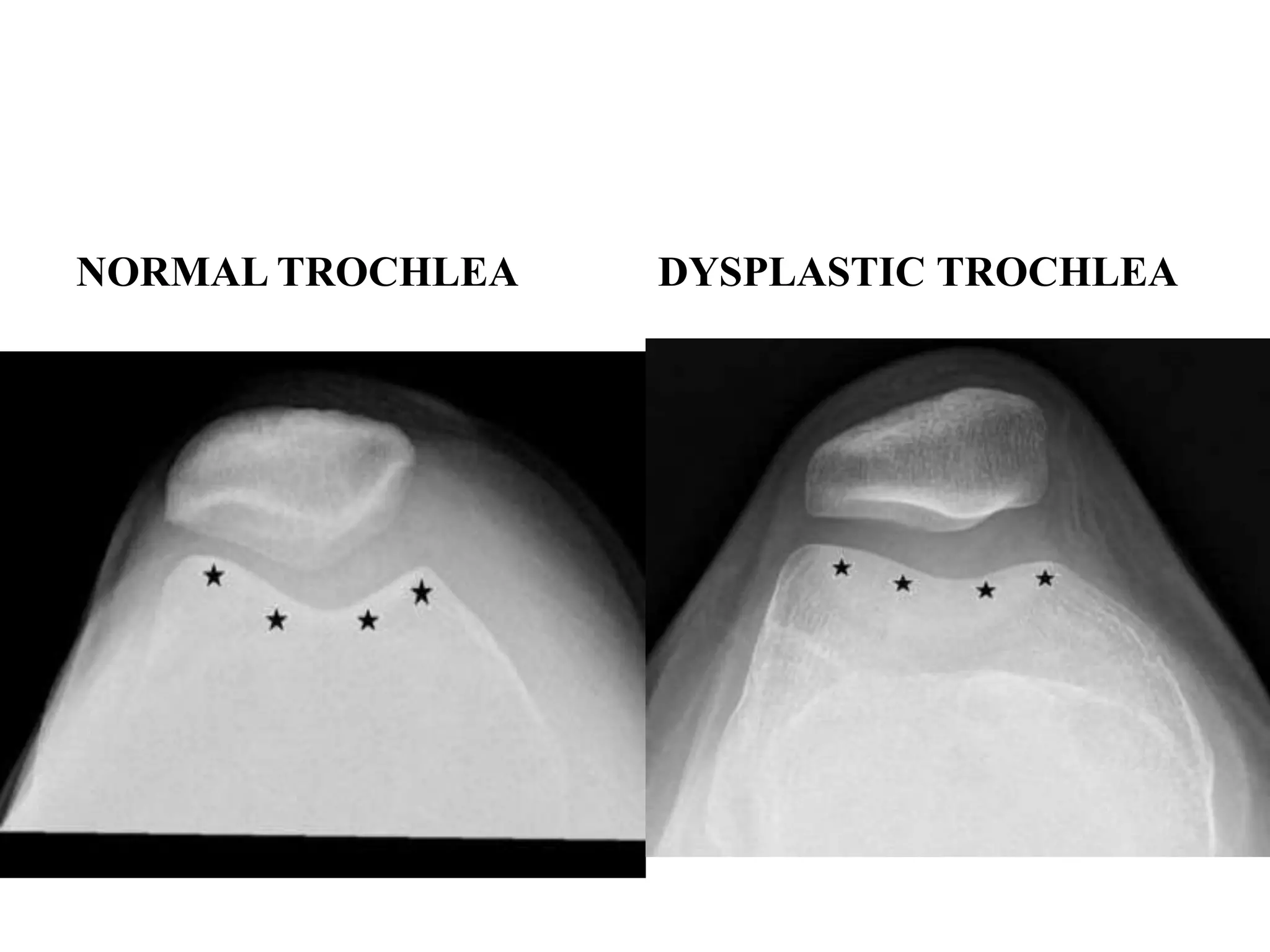
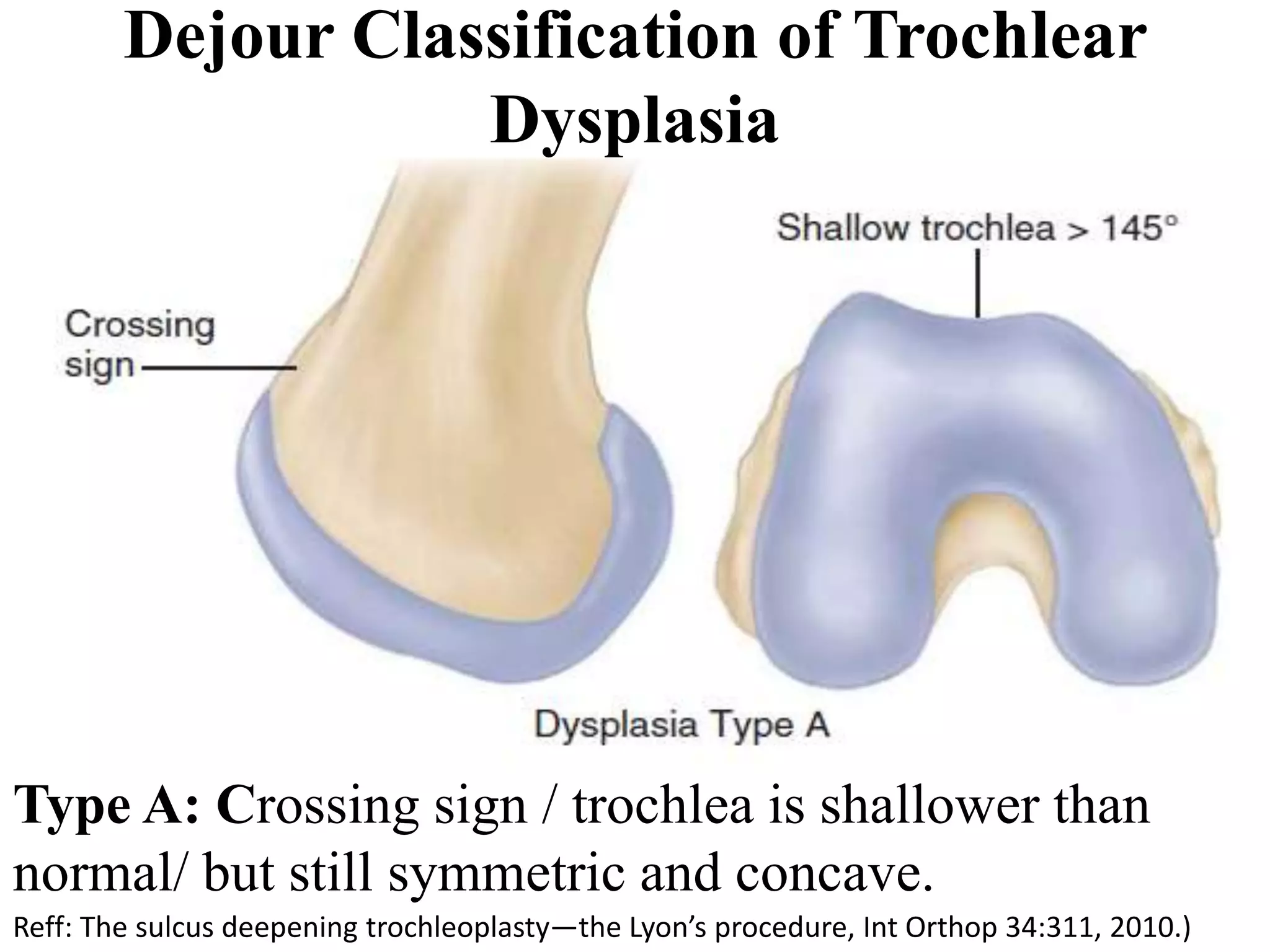




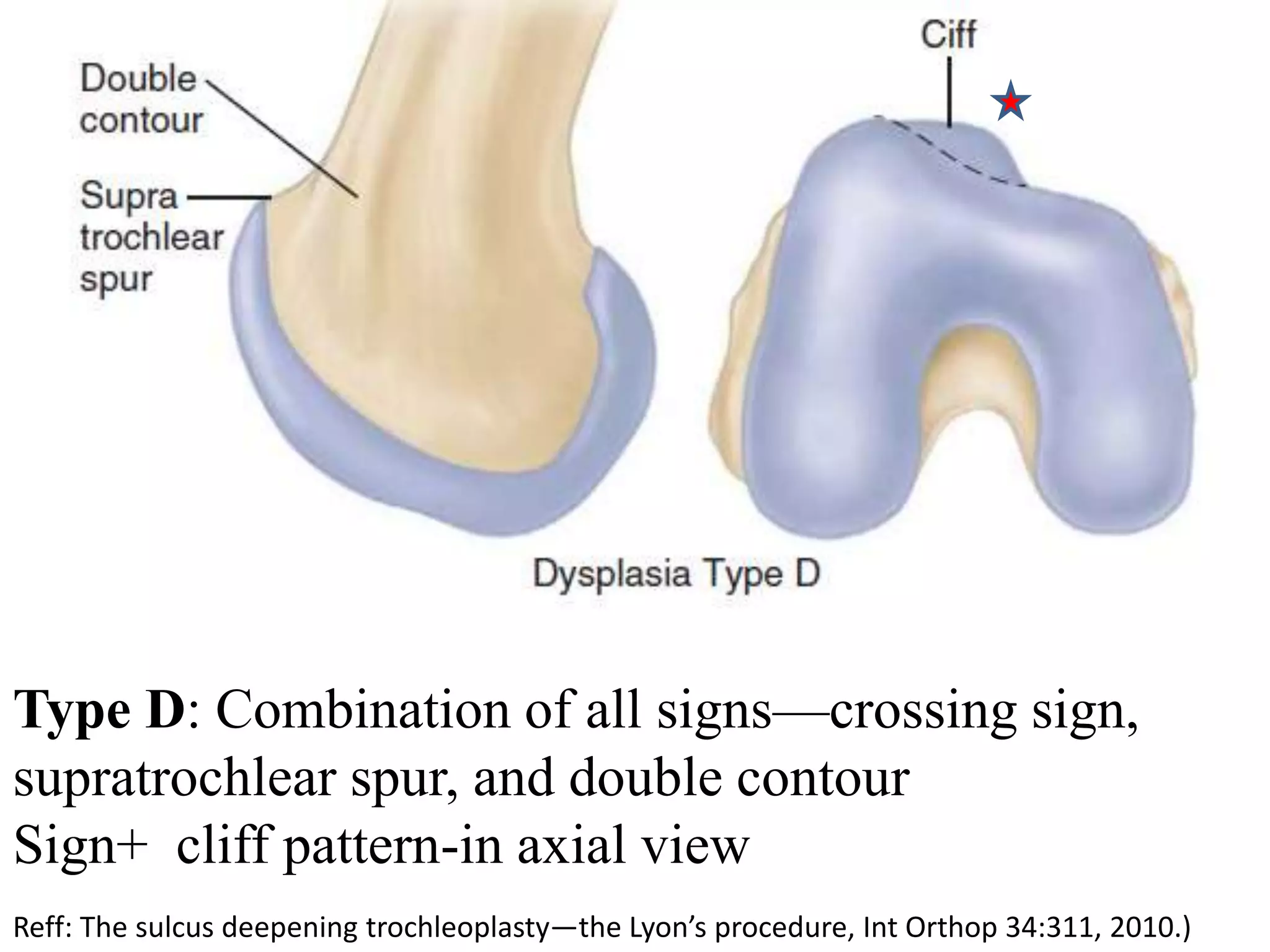




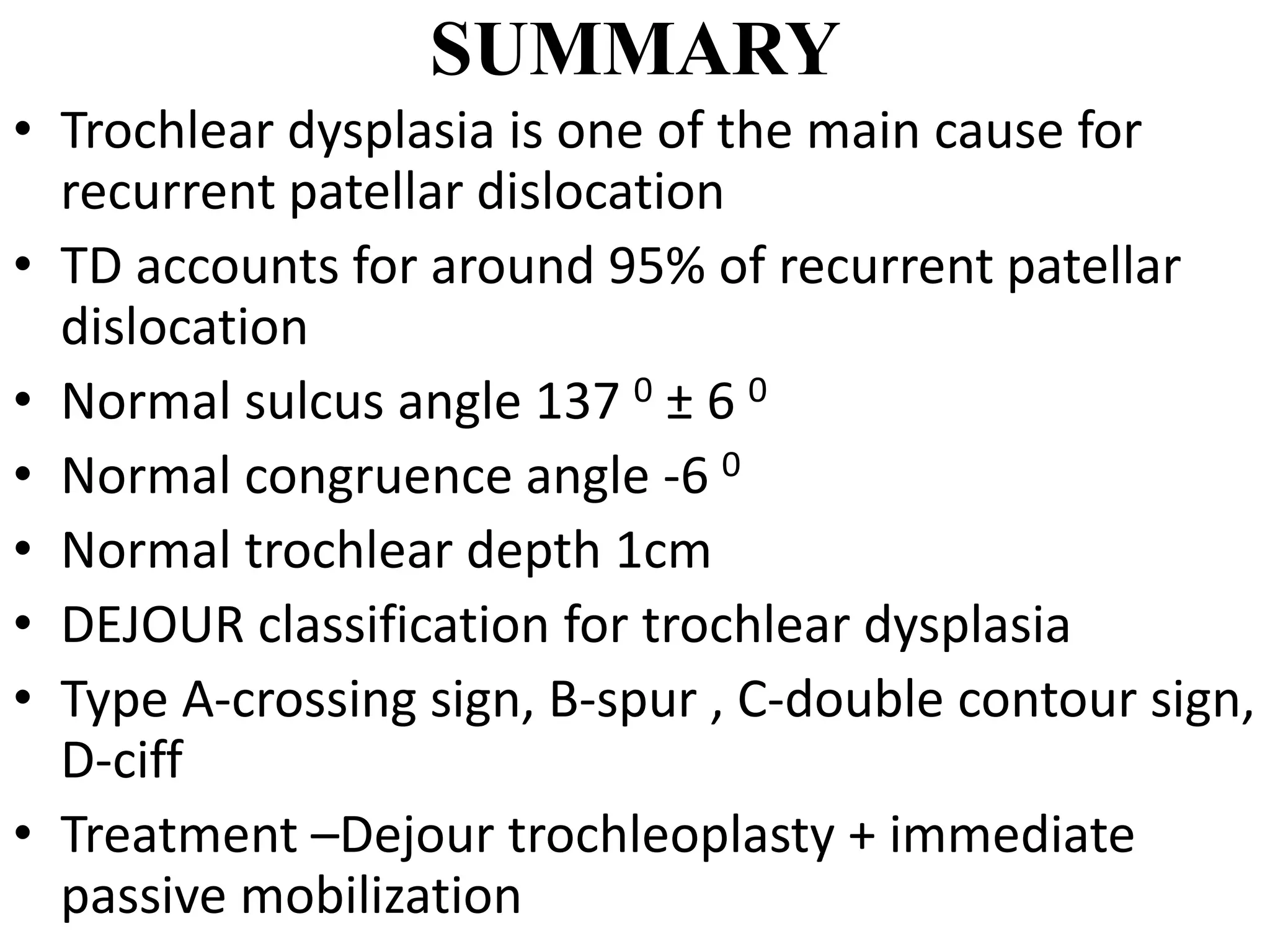
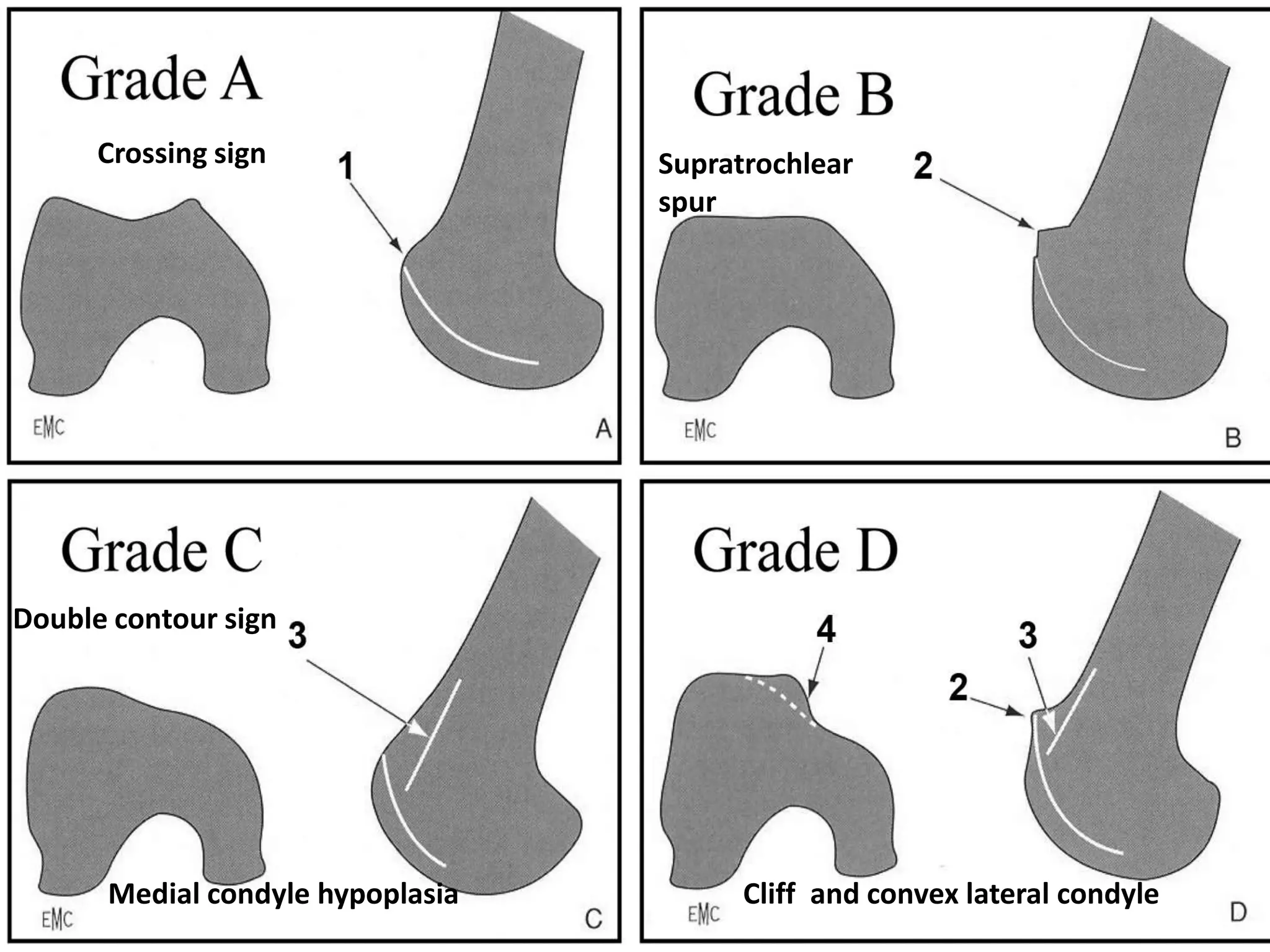


This document summarizes a lesson plan about trochlear dysplasia presented by Dr. Madhavan. The key points covered include: 1) Anatomy of the trochlear groove and how variations can lead to maltracking. 2) Classification of trochlear dysplasia according to the Dejour system from Type A to D based on radiological findings. 3) Treatment options like MPFL reconstruction and Dejour trochleoplasty to correct the anatomy in severe types of trochlear dysplasia.











































































