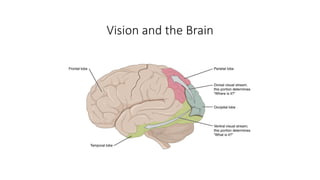
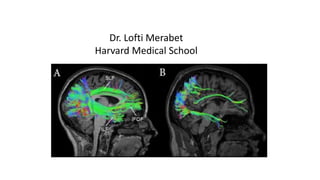
The document discusses cortical visual impairment (CVI) in children with Rett syndrome and related disorders, highlighting challenges in visual processing and the associated characteristics of CVI. It emphasizes the importance of assessment and tailored interventions to enhance visual function and learning through strategies and environmental adaptations. Key characteristics of CVI, assessment methods, and potential supports for parents are also outlined.