Downloaded 18 times

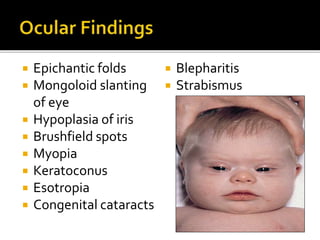
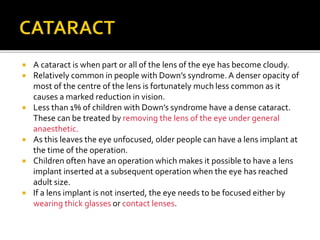

Down syndrome is caused by an extra chromosome 21. It has several characteristic physical features and causes intellectual disabilities. Eye problems are very common in Down syndrome, including squints, refractive errors like myopia and astigmatism, and eye infections. Regular eye exams from birth are important to monitor vision and treat any issues early. Common treatments include glasses, eye muscle surgery, and occasionally cataract surgery.










































![OCULAR EMERGENCIES IN PEDIATRICS [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/ocularemergenciesinpediatricsautosaved-240430020133-f6bf2643-thumbnail.jpg?width=640&height=640&fit=bounds)































