Downloaded 95 times

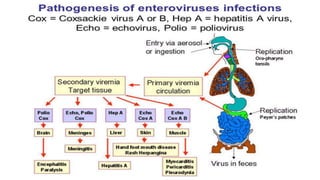


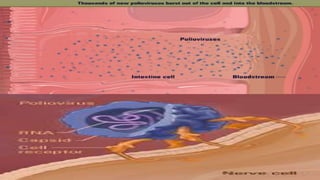
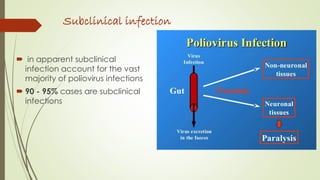


The document discusses viral gastrointestinal infections, specifically focusing on polio and echoviruses, which can be confined to the GI tract or spread to other body parts. It details the characteristics, transmission routes, and types of infections caused by these viruses, as well as prevention methods such as vaccines. Epidemiology data show that poliovirus is endemic in certain regions, while echovirus causes various opportunistic infections, particularly in children and immunocompromised individuals.



















































![viral_intestinal_infections._Clinical_and_lab_diagnosis[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/viralintestinalinfections-250319043604-bc7589f4-thumbnail.jpg?width=640&height=640&fit=bounds)



















![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)






