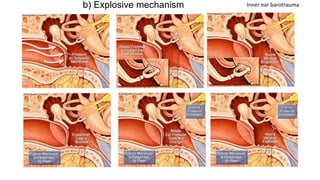
This document summarizes otitic barotrauma, which refers to injuries to the ear caused by pressure changes during diving or flying. It discusses the history of diving and describes the three main manifestations of barotrauma: sinus/middle ear issues, decompression sickness, and arterial gas emboli. It then covers the physiological effects of pressure changes on descent and ascent, outlines different types of ear barotrauma injuries, and provides treatment recommendations.