Downloaded 73 times



1. A 29-year-old woman experienced sudden loss of vision in her right eye and worsening neck pain after undergoing cervical manipulation by her chiropractor. 2. MRI revealed a right cerebellar hemisphere infarct and a left mesial temporal infarct, as well as a signal within the right vertebral artery consistent with an intramural hematoma. 3. She was diagnosed with vertebral artery dissection causing distal posterior circulation embolization and stroke. The manipulation likely dislodged a clot from a pre-existing vertebral artery dissection.

























































































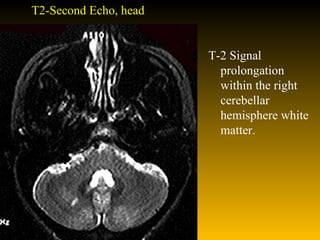
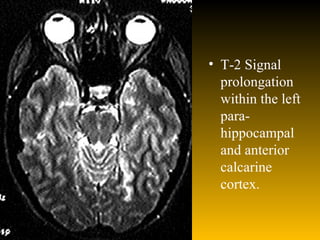
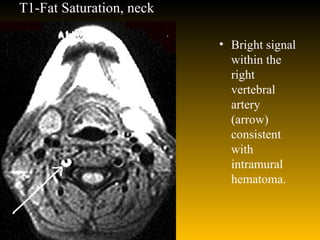
![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)

![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)



