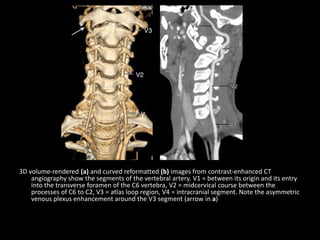
Downloaded 975 times

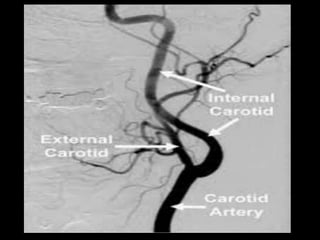
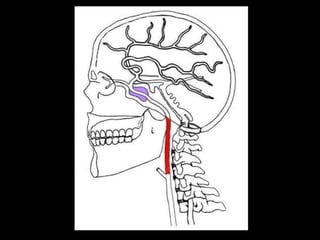


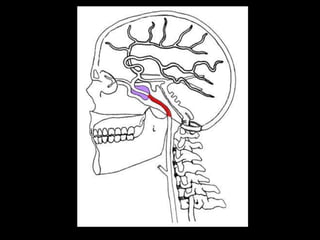

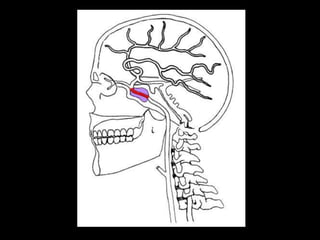
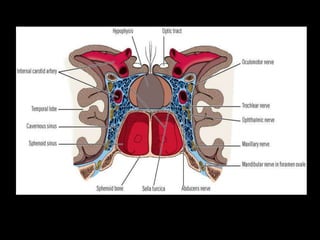
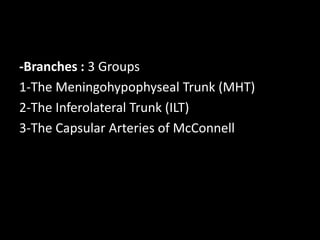
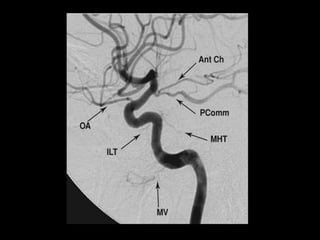
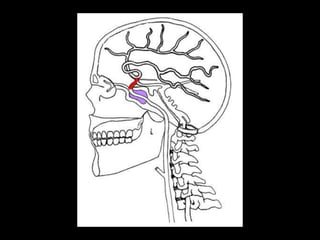
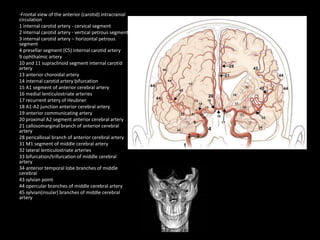
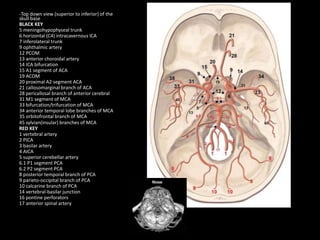
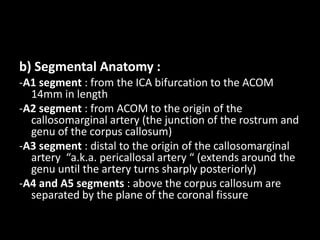
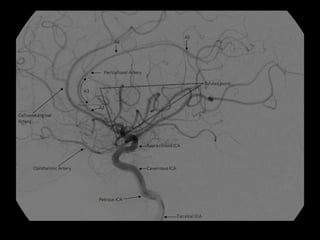
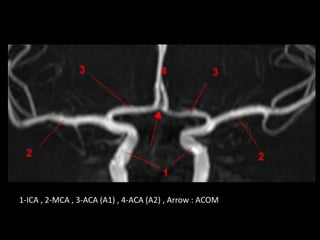
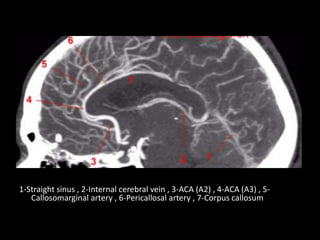
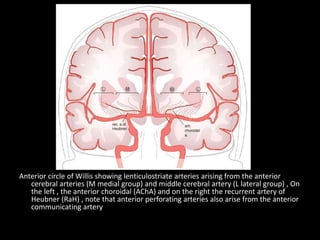
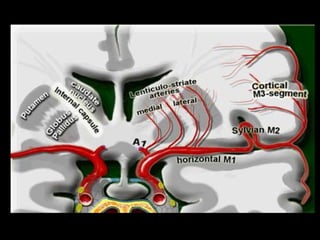
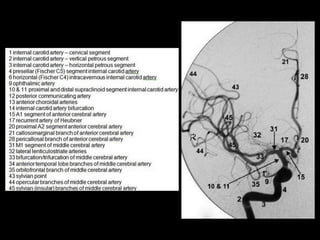
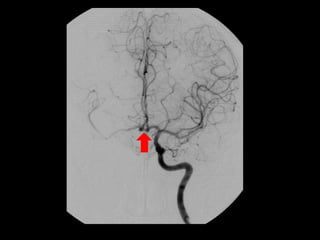


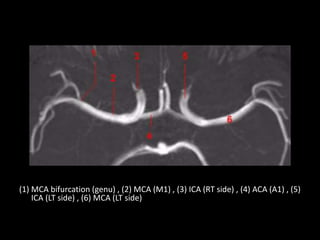
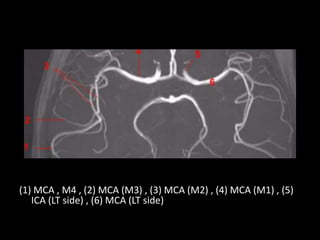
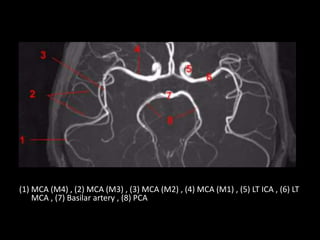
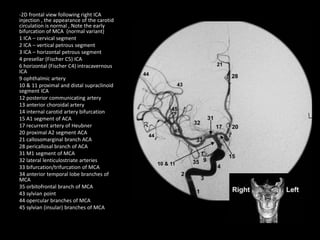
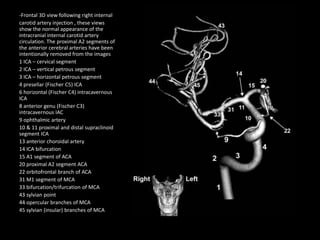
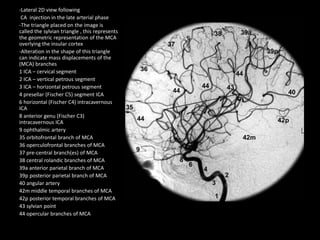
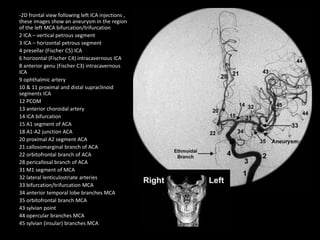
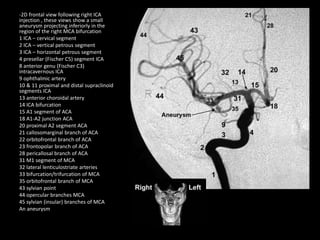

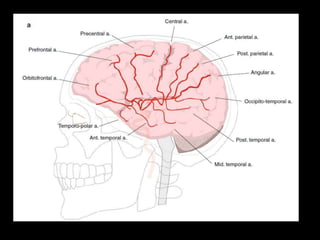
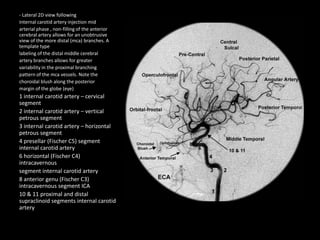
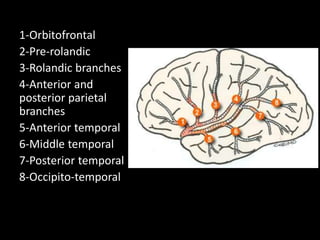
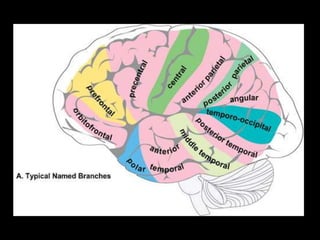
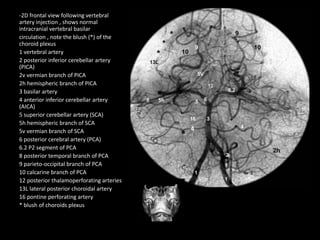
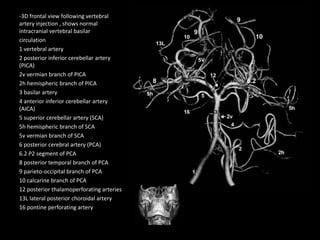
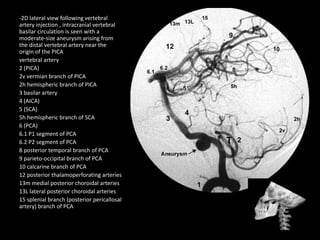
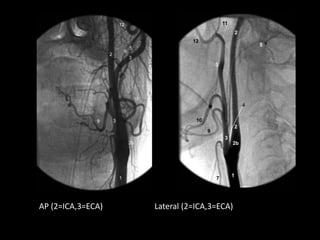
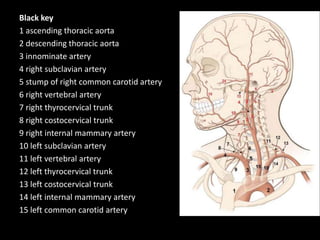
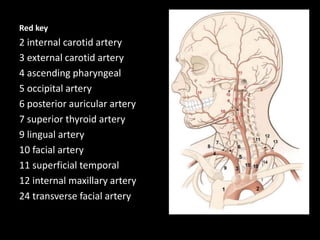
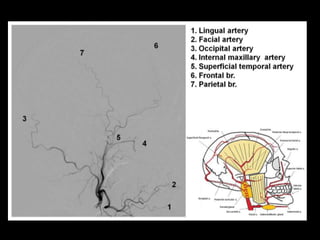
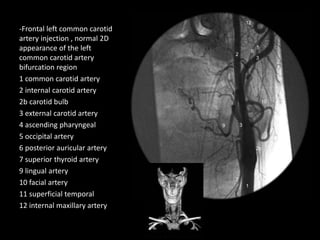
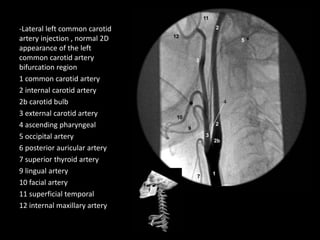
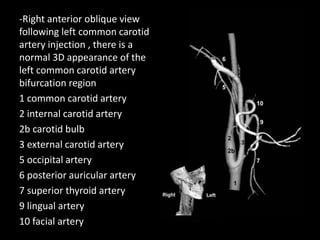
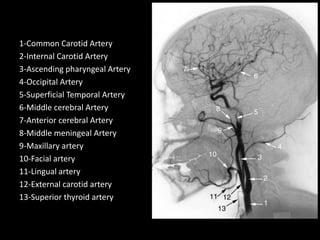
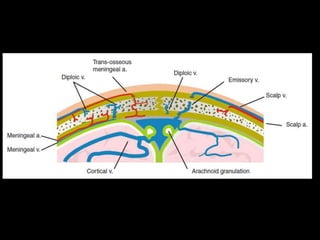
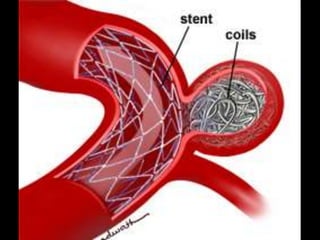
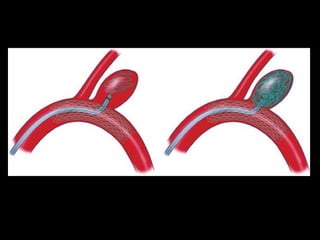




The document discusses the cerebral vascular anatomy, focusing on the internal carotid artery (ICA) and its segments, including the cervical, petrous, cavernous, and intradural portions. It outlines the origins, anatomy, and branch segments of the anterior cerebral artery (ACA) and middle cerebral artery (MCA), detailing their relationships and key branches. The information emphasizes the significance of understanding these vascular structures for successful disease management in interventional radiology.

















































![Vascular anatomy of head, [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/vascularanatomyofheadautosaved-181218123734-thumbnail.jpg?width=640&height=640&fit=bounds)











































