This document provides an overview of ventricular arrhythmias including:
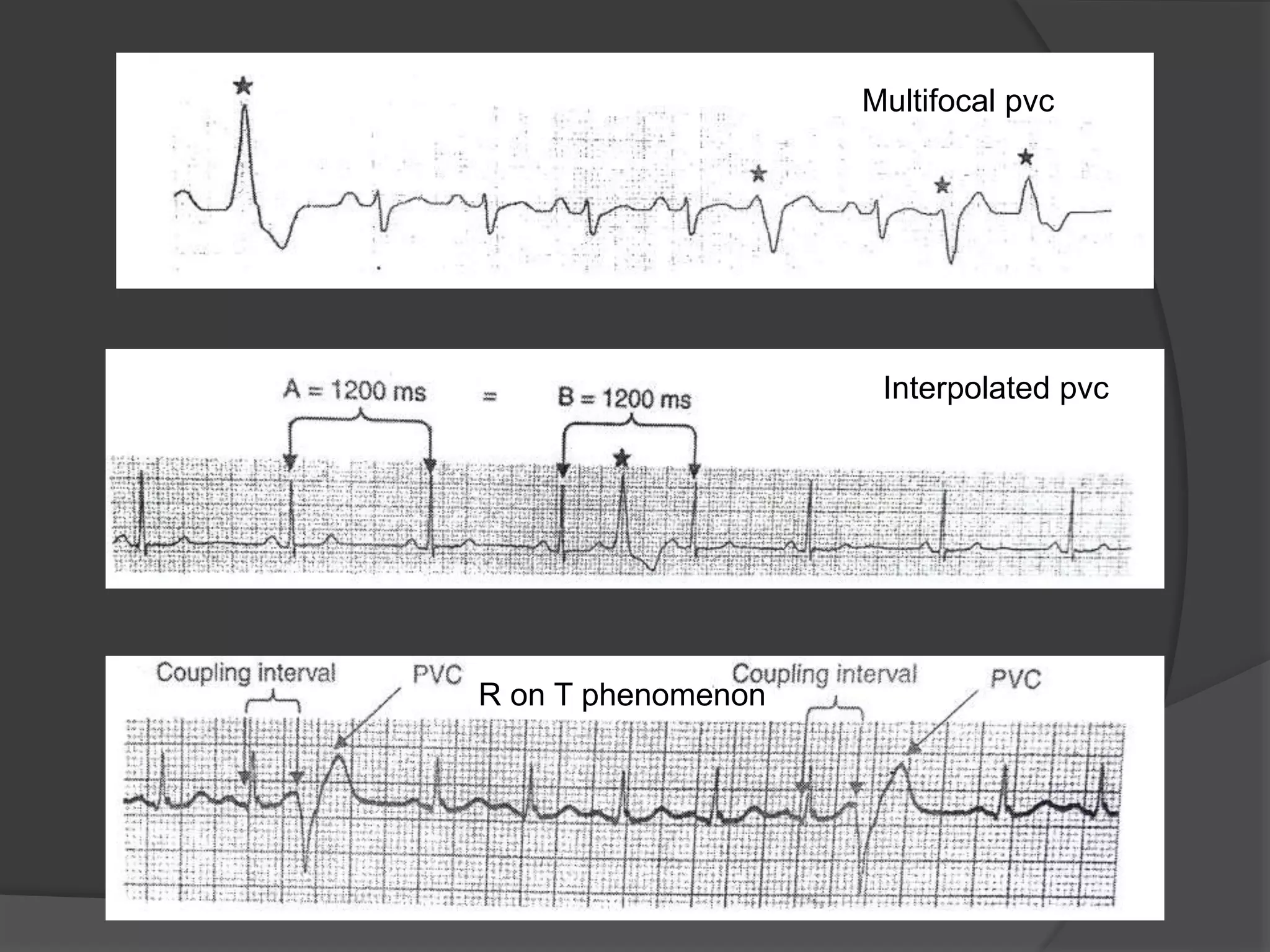
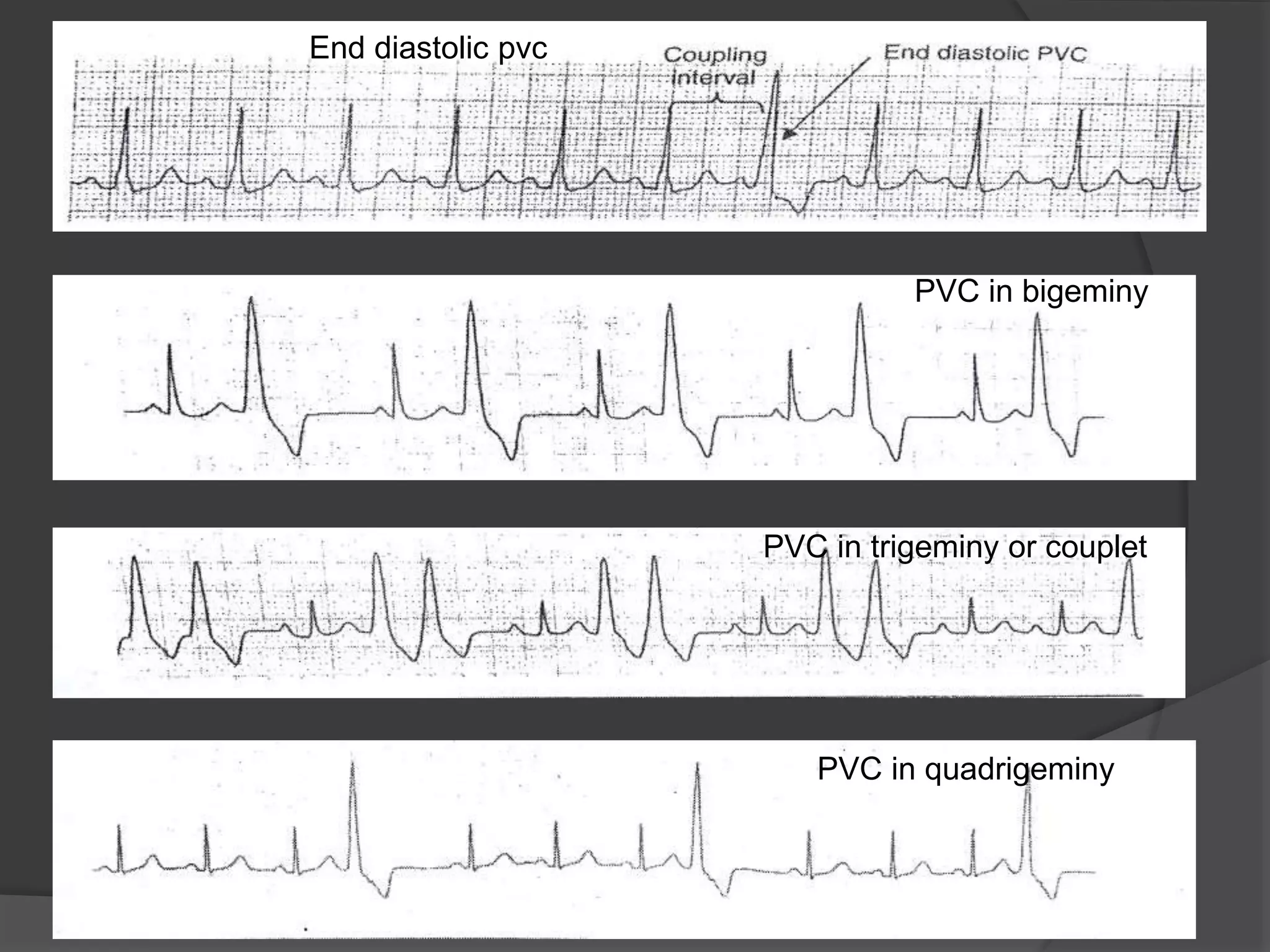
- Definitions of premature ventricular contractions and different types such as multifocal PVCs.
- Classification of ventricular arrhythmias as clinical (hemodynamically stable or unstable) or electrocardiographic (non-sustained VT, sustained VT, etc).
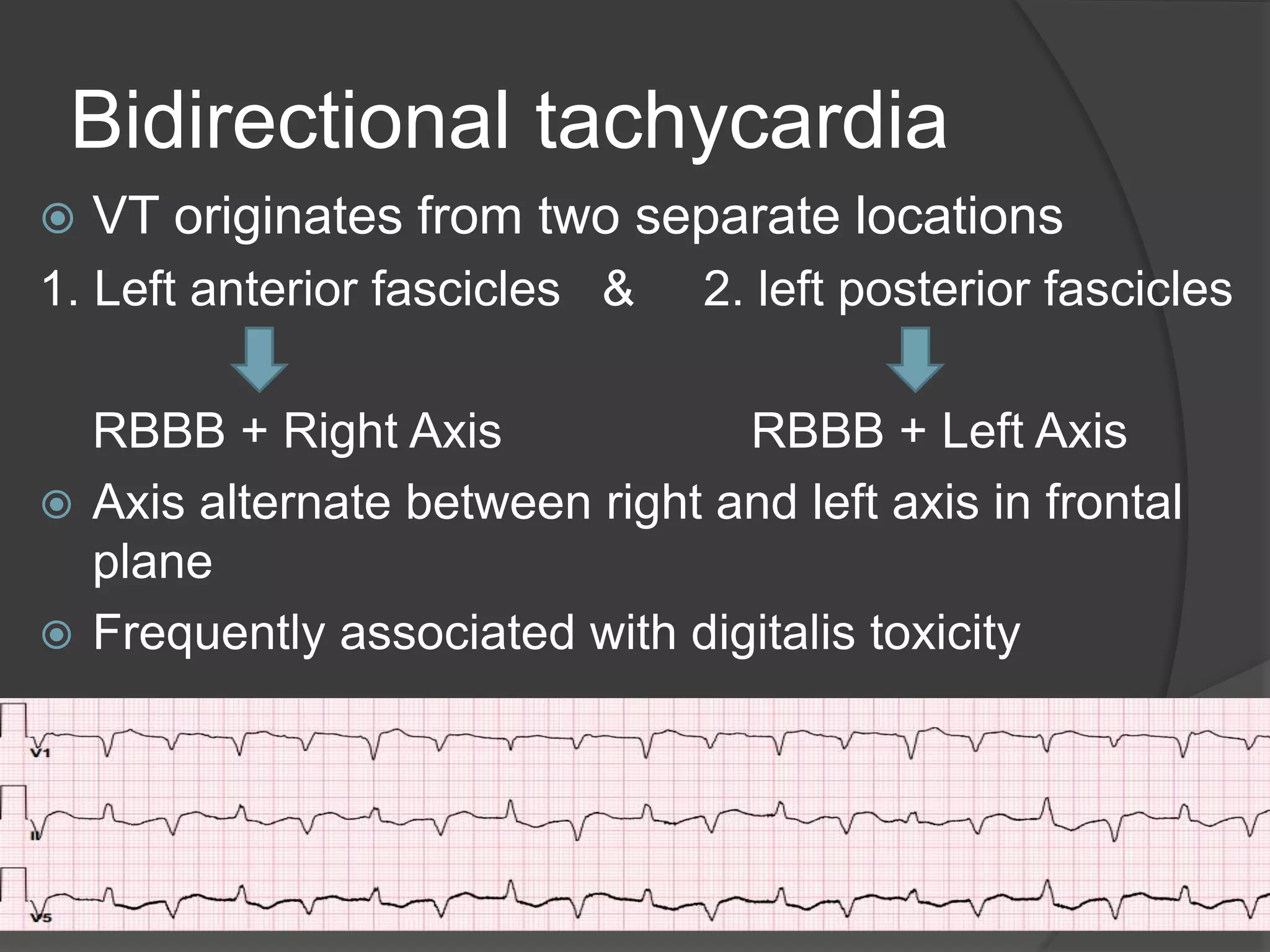
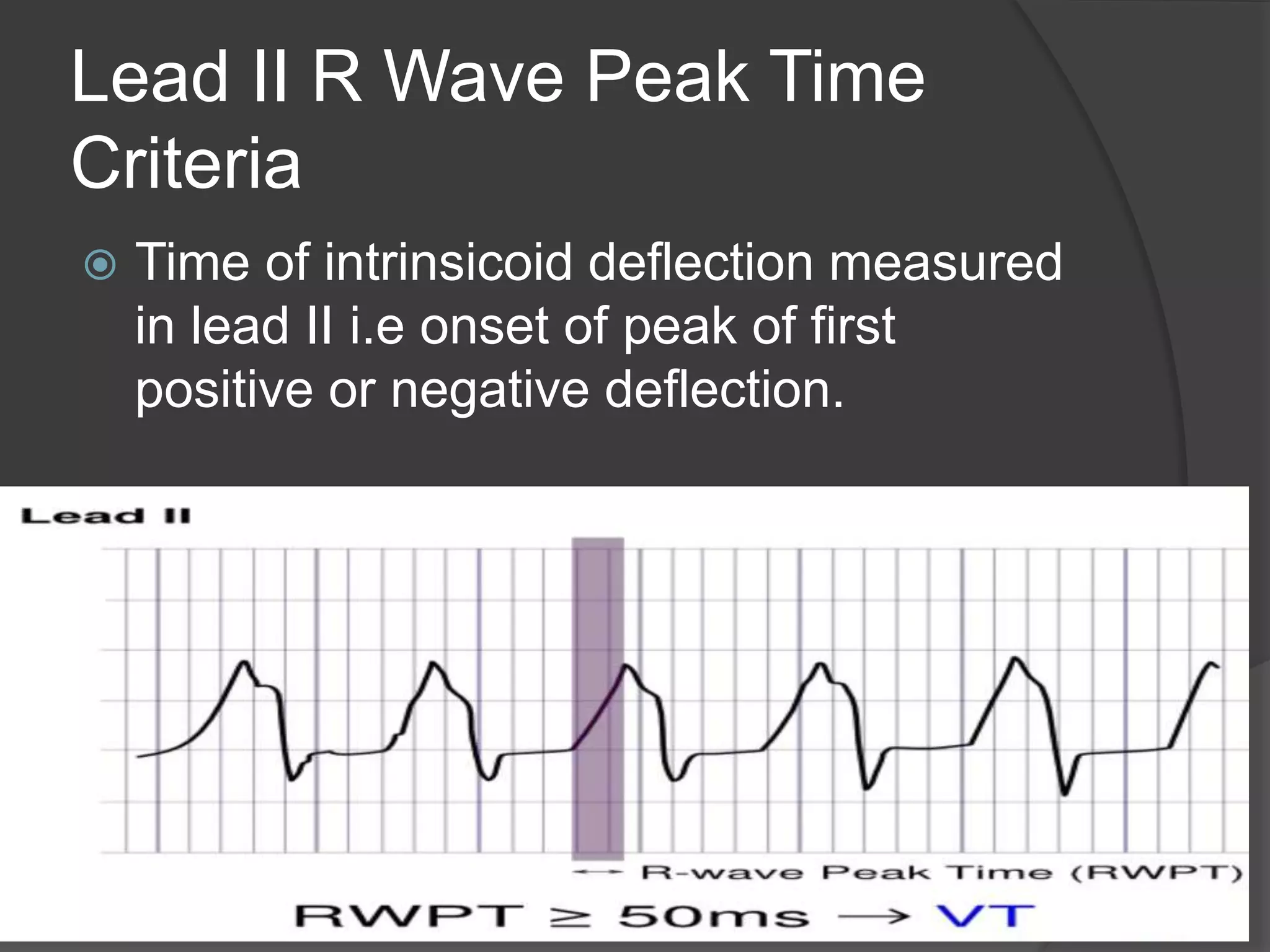
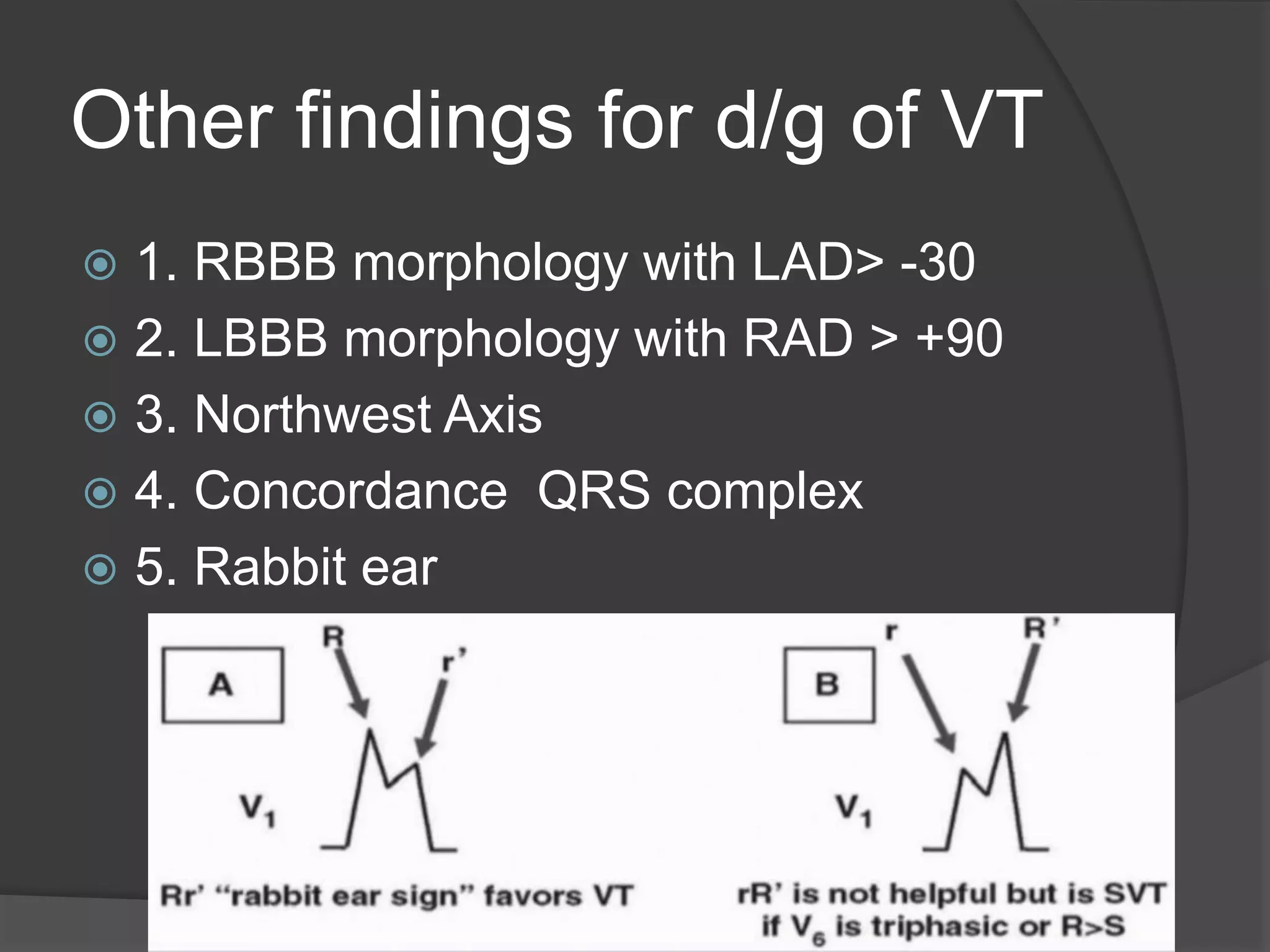
- Diagnostic criteria and algorithms for distinguishing ventricular tachycardia from supraventricular tachycardia using features on ECG such as AV dissociation, QRS morphology, lead aVR criteria.
- Treatment guidelines for ventricular fibrillation, sustained monomorphic VT, and polymorphic VT according to ACC/AHA/ESC guidelines.