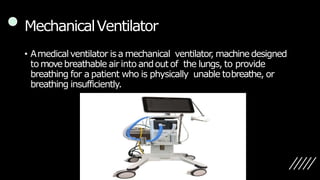
This document provides information on mechanical ventilator care. It discusses the purpose, equipment, types (invasive and non-invasive), modes, settings, and management of patients requiring mechanical ventilation. Key points include the goals of mechanical ventilation are to maintain effective ventilation and prevent complications. Modes of invasive ventilation discussed include volume control, pressure control, and pressure support. Settings that must be monitored and adjusted include tidal volume, respiratory rate, PEEP, FiO2 and more. The document also covers weaning a patient off the ventilator.