


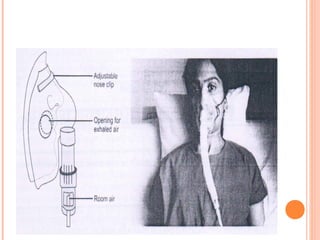


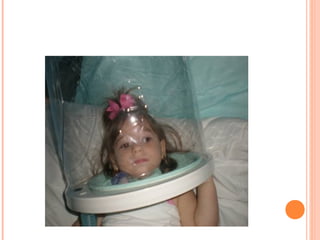





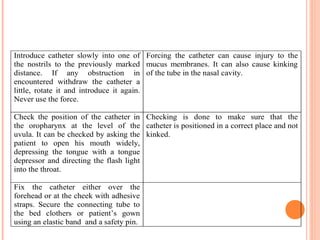


Oxygen therapy involves administering supplemental oxygen to patients through various delivery methods like nasal cannulas, masks, and tents. It is used to treat hypoxemia by relieving symptoms, facilitating tissue metabolism, and reducing arterial oxygen deficiencies. Potential complications include infections, collapsed alveoli, oxygen toxicity, and drying of mucous membranes. Proper technique is required to safely deliver the prescribed flow rate of oxygen via the appropriate interface while monitoring for complications and therapeutic response.

















































































