Downloaded 142 times
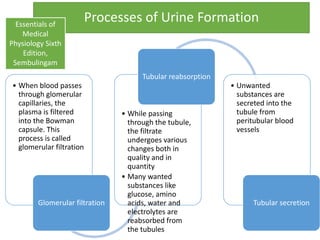
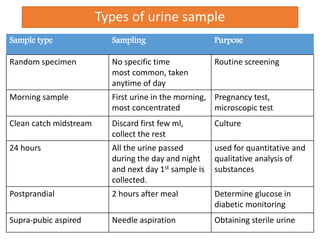
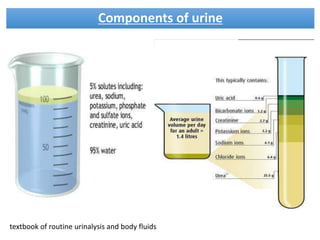
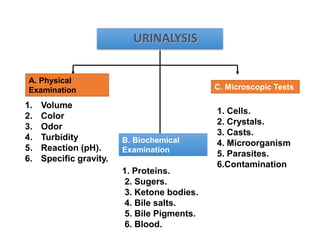
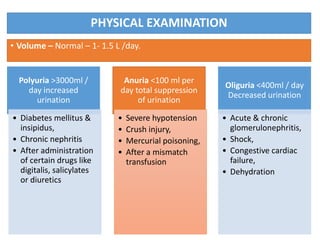
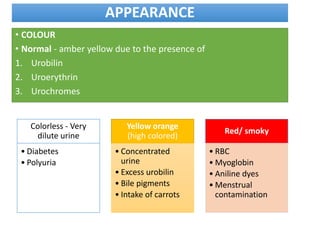
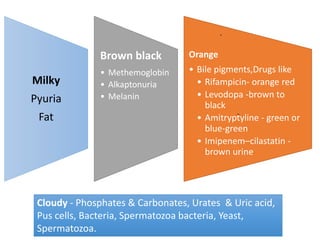
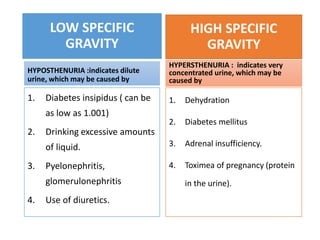
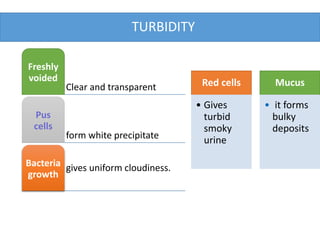
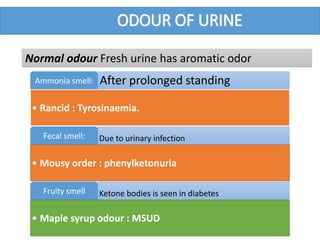
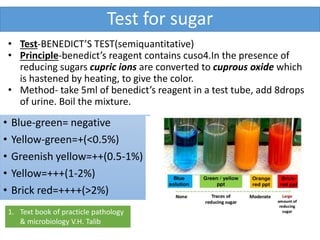
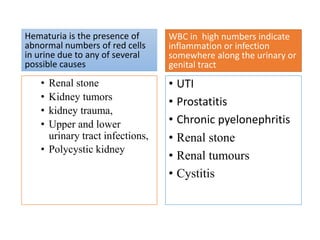
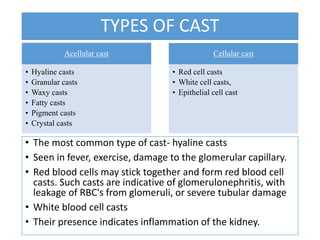
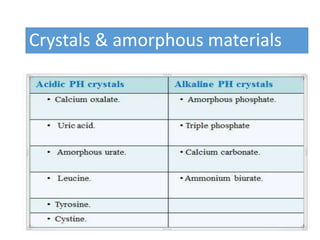

This document provides an overview of urine analysis in dentistry. It discusses the processes of urine formation, reasons for performing urinalysis, sample collection methods, and the components evaluated in a urinalysis. Physical examination assesses volume, color, odor, turbidity, pH, and specific gravity. Biochemical examination tests for proteins, sugars, ketone bodies, bile, and blood. Microscopic tests identify cells, crystals, casts, and microorganisms. Together these evaluations can help diagnose and monitor diseases affecting the kidneys, urinary tract, and other body systems.










































































