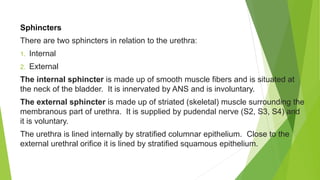
The urinary system consists of two kidneys, two ureters, a urinary bladder, and a urethra. The kidneys filter waste from the blood to produce urine. Urine travels from the kidneys down the ureters into the bladder, where it is stored until excretion through the urethra. Each kidney contains approximately 1-2 million functional filtering units called nephrons, which help regulate fluid and electrolyte balance and remove wastes from the bloodstream.





























































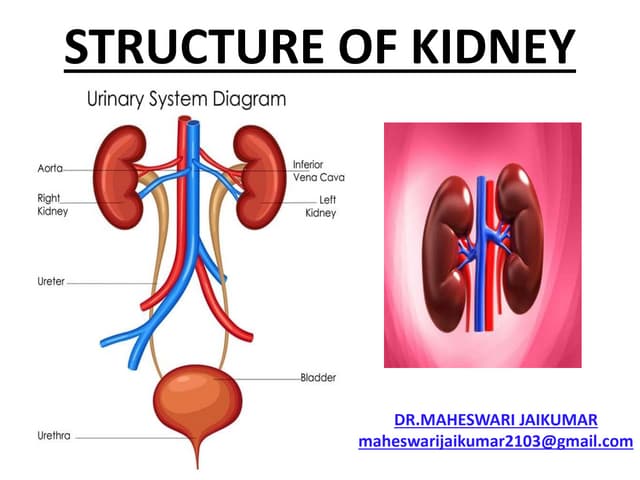
![Control of Water Excretion
Role of ADH
In general, increase in ECF volume inhibits ADH secretion, whereas decrease in
ECF volume stimulates it. However, major stimuli for ADH secretions are: plasma
hyper-osmolality and hypovolemia. Therefore:
a. 1% to 2% increase in plasma osmolality stimulates osmoreceptors (located in
the anterior hypothalamus); and
b. 10% decrease in effective circulating blood volume + decreases firing from
Baroreceptors (venous and arterial).
(a) and (b) → ↑ ADH secretion → directly ↑ permeability of DCT and collecting
tubules to ↑ water reabsorption
Key Point Since the plasma (Na'] accounts for 95% of the effective osmotic
pressure, therefore, in general, the plasma [Na] is the primary determinant of
ADH secretion](https://image.slidesharecdn.com/urinarysystem-220725102714-deb584b2/85/URINARY-SYSTEM-pptx-70-320.jpg)






























![The nervous system[1]](https://cdn.slidesharecdn.com/ss_thumbnails/thenervoussystem1-100413143207-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)
























































![Review of literature [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/reviewofliteratureautosaved-230315053854-fbe61789-thumbnail.jpg?width=640&height=640&fit=bounds)




















